Little Charlie was born full term via normal delivery on July 11th 2015. He is our fourth child and we were all besotted with him.
Soon after Charlie was born I noticed his back was a ‘funny shape’, but I was afraid to say to anyone in case my fears came true. I was so anxious inside.
When Charlie was just 3 months old my husband was feeding him, and while burping him he noticed his back just wasn’t right. He told me his concerns and it was at that moment my fears became reality.
We saw the pediatrician at our local hospital who agreed that Charlie’s back looked ‘off’, and she arranged an X-ray for him. After the X-ray I was brought into the pediatricians office. I could immediately see on her screen that there was a curve in Charlie’s spine. I was absolutely devastated.
We were then referred to the main Orthopedic hospital in Northern Ireland and we were advised to watch and wait for the next 3 months.
Three months passed and we were back for repeat X-rays to see if the curve in Charlie’s spine had progressed or not. He was just 7 months old, and X-rays showed his curve had progressed from 28 degrees to 42 degrees in just 3 months. We were absolutely devastated. All I could think about was “Charlie needs his little spine to grow”.
We were told Charlie needed to go into a plaster jacket that would be changed under general anesthesia every 6 months, until he would be old enough for the first of many invasive spinal surgeries. We cried for days. We never wanted this for our baby.
Once the news sunk in, we began to research. We wanted to see what the plaster jacket would look like. After joining the Infantile Scoliosis Outreach Programs (ISOP) Facebook Group, I quickly saw there were different types of casts! That’s when I began to question what these differences were. ISOP’s Facebook Group taught me that some casts are designed to hold the curve while others are designed to correct the curve gently.
For us, it was a no brainier. We had to choose MGGC. We wanted to try to correct the curve in Charlie’s spine, and potentially avoid him needing surgery.
After many phone calls, emails and endless days and nights of research, we soon realized that MGGC was not offered here in the U.K. or Ireland. The closest hospital to offer this treatment was Shriner’s Hospital for Children in Philadelphia, USA.
Yes it was a huge distance, but we were willing to do whatever it took to give Charlie the best chance to avoid invasive spinal surgeries.
Thankfully after a very speedy application and approval process, Charlie was accepted for treatment at Shriner’s Philadelphia.
We traveled from Ireland to Philadelphia in April 2016 when Charlie was just 9 months old. We met with the incredible team who would be treating Charlie, and we instantly felt a huge relief knowing he was in the hands of an experienced Doctor who specialized in Early Onset Scoliosis and Mehta Casting.
Charlie had an MRI of the full spine which thankfully came back normal, and he was ready to begin treatment. His curve was now 45 degrees, and he got his first cast under general anesthesia. As parents it was a shock for us to see our tiny little baby wrapped in a plaster cast. But after the first day we soon realized that this special cast wasn’t going to hold Charlie back from meeting his milestones and doing what he wanted.
Over the next 2 years and 2 months Charlie received a series of 12 Mehta casts all under general anesthesia. We would fly back and forth across the Atlantic every 8 weeks so that Charlie could have a new cast applied.
Throughout his treatment he had regular X-rays to check how his spine was responding to the casts.
In June 2018 we received the news that we had hoped and prayed for, that Charlie’s curve was down to 9 degrees standing out of cast with a fully relaxed spine. We were just bursting with joy.
Charlie then graduated to a full time brace which he would wear for 23 hours a day until he would outgrow the brace. Over the next 2 years and 4 months Charlie a total of 3 full time braces. And in October 2020 it was agreed that Charlie could move to night time only bracing because his spine was holding at 8 degrees.
For the next 9 months Charlie enjoy his new found freedom during the day, and continued with bracing at night. He then began to outgrow his brace, and we decided to X-ray him in Dublin Ireland and send the results across to Charlie’s Doctor at Shriner’s.
To our amazement Charlie’s spine was completely straight! There was no measurable curve! This was the day we had hoped and prayed for since our journey with Charlie began. Charlie was finally cast and brace free for the first time in over 5 years.
Its been 13 months since Charlie was last in brace, and he is still monitored by X-ray every 6 months or so. At his last check he was still holding steady.
We will be forever grateful to Dr Min Mehta for developing this gentle non invasive treatment to help guide our little warriors to grow straight.
Her global work as a pioneer in championing straight spines helped save the lives of countless babies with Progressive Infantile Scoliosis
For thousands of families across the world and for ACCO, 2005 was one of those remarkable times when we experienced a significant sea change in the treatment of very young children with a diagnosis of life threatening Progressive Infantile Scoliosis.
In 2001 we became acquainted with Heather Hyatt, mother of a beautiful four year old named Olivia, who initially reached out to us to help her find a preschool program for her precious child diagnosed with severe Progressive Infantile Scoliosis. At the time, Olivia had already undergone halo procedures. However, Heather never accepted that a single intensive, invasive and premature procedure of spinal fusion surgery was the only way to treat Olivia’s condition. With courage and determination, Heather began an international search for a cure, and through her perseverance, her journey lead her to the extraordinary and brilliant Dr. Min Mehta, a Pediatric Orthopedic Surgeon from London. We were unbelievably fortunate to have Olivia join our program and Heather has taught us that nothing is stronger than a parents love for their child. Unfortunately, Olivia was too old to benefit from Dr. Mehta’s technique, but she has taught us all a lesson in what true strength looks like. As many of you know, we lost Olivia in February of 2016, however, she will always be remembered in our hearts as the inspiration for the Infantile Scoliosis Outreach Program (ISOP). Olivia and her story will not be forgotten.
When Heather met Dr. Mehta, who suffered from juvenile scoliosis, she was pioneering a noninvasive procedure to cure vulnerable babies with Progressive Infantile Scoliosis. Over the last 12 years, this initiative, spearheaded by Heather, became an established program of ACCO, which has developed into a global effort, spreading knowledge, defining better options for families and organizing free, hands-on training for hundreds of doctors and others on Mehta’s Growth Guidance Casting, resulting in thousands of babies being cured gradually without dangerous surgery.
Dr. Min Mehta left us in August 2017 and while there is no way to adequately express the heartfelt gratitude we feel, we understand how incredibly fortunate we were to have known her and what an honor it has been to work with her. Dr. Mehta once said that, from the age of six, she had always wanted to be a doctor, and she faced enormous challenges, including a negative and dismissive perception of women in the medical field. However, this gentle, non-invasive technique would not have been possible without her significant life’s work, and we know her enormous impact will continue to spread around the world. Heather, as well as many others that knew her, have heard so many life changing and grateful stories from parents and the medical community about the unbelievable impact that Dr. Mehta has had. She is considered the global authority on the only life threatening condition in the world of pediatric orthopedics.
For her compassion and dedication to making the world a better place and for her legacy, which she has left for everyone that has been touched by Progressive Infantile Scoliosis, Dr. Mehta will be forever missed but will never be forgotten, nor will the lifesaving work that ISOP will continue to spread until no more children suffer like Olivia and many others with this devastating, painful and life shortening condition.
I cannot thank you enough, from the bottom of my heart, for how grateful we are.
You are a special person and to get such precise information to us so quick and feeling poorly.
We have a fight on our hands but will will fight and get the best treatment for _____.
Its people like you that make this world a great place to live in.
I will keep you updated and once this has been sorted I will be looking at some point in the future to
highlight infant scoliosis in the UK. Im not sure how but have a group of parents who are up for a bit
of positive media coverage also.
If you are ever in the UK you are welcome in our home.
Ryan, our wonderful surprise baby, was born just 11 months after his bother. I had no complications during my pregnancy and Ryan was born to term. Ryan was always laid back and happy. Other than some reflux, he was very healthy. We did notice some differences between Ryan and his older brother. Ryan learned to sit up later than his brother and when he did, he had bad posture. He slouched, and he would plop down and lean back on his little Mickey Sofa. Sometimes he would just stop playing suddenly and lay down. I used to joke and say he was being lazy. Shortly after his 1st Birthday, I noticed the ribs on the right side of his back were sticking out. It looked like he had more muscle on that side of his back. I showed my husband and we both knew something was wrong.I got him in to see his pediatrician’s associate. He didn’t seem too concerned, but after I mentioned that Ryan’s older sister had to have surgery for her severe scoliosis at age 12, he told us to have x-rays taken. My husband took him to get his x-rays the next day at a local lab. My husband said that when they took the x-rays, Ryan was laying down; my husband held Ryan’s legs straight, while the tech pulled his arms above his head. This first x-Ray, measured Ryan’s curve at 17 degrees. That night my husband showed me the x-ray and told me that it Ryan has what’s called Infantile or Early Onset Scoliosis. I immediately started searching the internet for information. Luckily, I came across the Infantile Scoliosis Outreach program. I read all about Mehta casting and saw the success stories. I joined the Early Onset & Mehta Casting Facebook group and read through every post I could. All of the parents were so helpful. I learned that Ryan’s curve would be worse than 17 degrees since he was lying down and pulled straight for the first x-ray. I learned that he needed a Mehta as soon as possible. He was already 13 months and the best window of time to cast is between 1 and 2 years old. I had also read that parents in our area were taking their children to the Texas Scottish Rite Hospital for Children in Dallas. By the next morning, I was on the phone with Heather Hyatt Montoya. She confirmed that Ryan needed to go to the Texas Scottish Rite Hospital soon. Our pediatrician referred us to the hospital but we were told we would need to wait for 3 months until out initial appointment. With Heather’s guidance, I put together a packet and sent it to the hospital. I was thrilled when we got a call within the week and got an appointment the next month.
At Ryan’s first appointment, proper standing x-rays were taken. The standing x-ray revealed Ryan’s curve was actually 34 degrees and his RVAD was measured at 29. An RVAD over 20 generally means it will progress. We set up a casting date for October 24, 2013. I was nervous for the first casting but I knew my little guys needed this treatment. The best news was hearing that the doctor was able to get great Ryan’s curve down to 11 degrees in cast number 1. Eight months later and Ryan is now in cast #4. His curve is measuring at 8 degrees in cast. He will get his last cast on July 11, 2014.
Ryan is thriving in his cast. He can do everything another toddler his age can do except get wet. He loves playing with his brother, jumping on his trampoline, and going on walks. He is happy, healthy and his spine is growing straight. We are so blessed to have found Heather and ISOP when we did. We are sharing Ryan’s story to show that Mehta’s EDF casting works! There are still so many pediatricians who don’t screen for infantile scoliosis and so many specialists that don’t recommend casting. I have heard from countless families who were told to “wait and see” which lead to these children missing their window for early treatment. Mehta Casting should be the first option for children like Ryan.
Just wanted to provide an update and thank you for your help in getting us headed in the right direction. Without ISOP we would have had no alternative but to wait six months as the ortho doc requested and our baby would have had a long road ahead of him without Mehta casting. We were able to get an appointment with Dr. ____, last Wednesday, and he recommended casting!
We go back in two weeks for his first cast and MRI. Everyone was so nice there and we are just overwhelmed by how blessed and grateful we feel to have found ISOP, had immediate access to and advice from you, and the general encouragement that is given and shared amongst the FB group. You are really doing something special and amazing, Heather. If you hadn’t fought so hard to get this alternative established so many families would not be having the experiences they are.
I don’t know how to repay you for the role you have played in our son’s future. I know we are just starting this journey, that cast #1 may be the hardest, and there are days when I have no idea how we are going to cope and get through it, but I know that we will. We will keep you and the FB group posted as we continue our journey but I just wanted to check in and most of all share my gratitude.
This is our child who is being treated with Mehta Method EDF plaster corrective casts for Progressive infantile Scoliosis. This video was shot approximately 24 hours after having his first cast applied at the Shriners Hospital in Salt Lake City, UT. We have uploaded it to show parents who are considering Early Treatment casting to correct and potentially cure Progressive Infantile Scoliosis how quickly children adjust to the cast. Please visit www.abilityconnectioncolorado.org/newsite/infantilescoliosis to learn more and visit www.girltomom.com to read more about Bexon’s story.
The moment Maggie was born we knew something was wrong. When the doctors quickly whisk your child away and whisper in a corner, things are probably not going well. She had severe torticollis on the right side of her neck, causing her face and ear to swell. While in the hospital she had a quick x-ray, renal ultrasound and echocardiogram – fortunately her heart and liver were functioning properly, although the x-ray revealed a 30 degree spinal curve.
Maggie was a small, full-term baby and a poor eater (Breastfeeding did not work). Even on breast milk she developed reflux, and gained weight very slowly. It’s funny looking back on those early days as her nutrition was our paramount priority. We even took her to a GI doctor and worked tirelessly to get food into her. While still very small (5 years, 27 pounds), our focus has changed significantly.
Pretty quickly after her birth we were at the orthopedic clinic at our local Children’s Hospital. The doctors said that usually infantile scoliosis resolves by itself in a few months. After a year the curve was at 50 degrees – Maggie was becoming noticeably asymmetrical. Our appointment schedule shifted to every 2 months, with a chest x-ray to assess the curve. Six months later, the number was at 60 degrees – the diagnosis was progressive infantile scoliosis. It was time to start treatment…
Maggie’s curve is very high in the thoracic region of her spine – a very hard place to treat. In addition, an MRI revealed no rib or vertebrae deformities. Her spine just wanted to curve. The recommendation was to start with a Risser cast to shape the spine through pressure on the ribs. It’s hard to explain the horrible feeling that washes over you as a parent to know that you “opted-in” to a bulky, hot and itchy torso cast. We took the week prior to the casting as a perfect excuse to go to the beach. Seeing Maggie in the cast after the procedure brought me to tears. Waking up from anesthesia as an 18 month old kid now stuck in a cast that weighs one third of your body weight was more than I could handle. Maggie handled it way better than I did – she was active, mobile, and more or less unaffected. Her spine also, was unaffected. Each subsequent visit to children’s revealed a small increase to the curve: 62 degrees, 66, 72, 75, 79, 81, 82, then 90 degrees. Maggie was amazingly not showing any ill affects of her curve; no shortness of breath, fatigue, or trouble walking. Still, casting was not working…
Our doctors introduced us to VEPTR, an extendable titanium rod which is implanted in the back to manage a spinal curve while a child is growing. Sounded like the holy grail to us. “My daughter gets to get out of this cast? Swim? Take baths? And the results are very positive??” Sign us up. Maggie was around three and a half by this time with no relent to her ever-progressing curve. “There’s another option as well” our doctor told us, ‘It’s called halo traction”. Horrified, we could hardly even comprehend the desperation required to engaged in that medieval torture. “You seriously have to drill a halo into her head? Then hang her from a pulley in a walker or wheelchair she can’t get out of???” It literally could have been one of the worst things I could imagine. “But it’s easily reversible, and isn’t major surgery.” said our Doctor. We though about that for 10 minutes and concluded: VEPTR it is….
Maggie’s surgery was scheduled a couple days after her fourth birthday. We told her staying in the hospital would mean as many movies as she wanted – she was very excited. The surgery took three hours, three nerve-wracking hours, full of pacing, staring at each other, and mindlessly surfing the internet. She metabolized the anesthesia very quickly, and woke up fast and disoriented in the PICU, without us there. When we were finally allowed back, it took my wife a long time to calm Maggie down. Sleeping in hospitals is the absolute worst: two days in the PICU, and 4 more in the recovery room put a huge strain on my wife, who would not leave. Maggie’s condition was sub-par, she was unable to move her right arm (fingers moved though), her pain was high, and we were discharged with her hardly walking. A slow couple of weeks saw her going back to preschool an hour at a time, and some increased right arm movement. Then everything went bad, very bad…
Maggie suffered an episode at school that put her in a great deal of pain. She stopped moving her right arm, had a great deal of asymmetrical sweating (only the right side of her face) and was unable to do much but sit on the couch. We thought it was a strain or a pain spike and that a good night’s sleep would make it better. It didn’t, her condition worsened. She was lethargic, scared, and extremely timid – her face resonated pain. Our doctors did not know what could be causing it, guesses included a muscle tear (they had to cut through many layers of muscle on the right side to seat the VEPTR), an infection, or nerve damage. We continued to hope that rest and minor physical therapy would improve her condition, it didn’t. This went on for a month, until her sutures burst on her back – infection was now the known culprit. Surgery was scheduled to clean out her VEPTRs – it was performed the next day. She was put on antibiotics and we were sent home. Her condition slowly but steadily improved and we took her off the antibiotics. After about a month, constant monitoring of the wound did reveal that the new sutures started to pull apart again, we went back on the antibiotics. The wound healed as did Maggie’s condition – she regained full movement of her arm, along with her bubbly personality. She was however on 3 doses of antibiotics everyday, with no real exit strategy other then pulling out the rods.
After the initial VEPTR surgery, Maggie had three extension surgeries. They had no positive effect. Her spinal curve was over 95 degrees – I think the doctors must stop giving you exact numbers at this point, as they started telling us “Mid to high 90’s”. That desperation I talked about above was now on us in full force. We started getting our minds prepared for the ‘medieval torture devices’ – it was the only reversible option left. We formulated a plan: We took Maggie off the antibiotics, and would let the infection tell us that it was time for the rods to come out and the halo traction to go on. The infection didn’t come back… Great, now we get to choose when Maggie goes in the wheelchair. We tried one more extension surgery with no improvement and quickly scheduled the halo traction surgery….
Maggie would be getting her rods pulled out and a halo attached to her skull with eight screws. I did not cry when I saw her after she woke up from anesthesia. Her halo was big and bulky, with a large metal hook to attach to the wheelchair/walker’s(forthwith referred to as ‘hardware’) pulley system. Fortunately, there was no need for the PICU, and we went straight to the recovery room. Three more nights in the hospital, but Maggie was doing really well – both in terms of her pain and her tolerance for the hardware. Two days after surgery she was running down the halls of the hospital in her walker, jumping and doing tricks on the pulley system and making friends in the playroom. I’m lucky I recently upgraded my Subaru Impreza to a Ford F150, I don’t know what we would have done trying to move the hardware in anything but a pickup. Due to the fact that we currently have only a few weeks of experience with halo traction, I’ll end on this positive note: After one week of halo traction, and only two days of the final traction weight, Maggie’s curve has gone from over 100 degrees to 66…
At the end of two months, Maggie’s curve is down to 50 degrees. It amazing for us to see some treatment actually have a positive effect. I feel horrible now that we even went through the VEPTR surgery, probably a regret I’ll have for the rest of my life. After the halo came off we had Maggie fitted for a new brace. One that has a neck brace along with a body brace – Maggie has been wearing that for about 23.5 hours per day. We’ll get another X-ray in a month to see how her spine looks, but the traction/bracing has given us new hope that we can keep her growing for a years to come.
At just five and a half months old, tiny little Nora was diagnosed with congenital scoliosis. We had noticed a curve in her spine; it was actually hard to see. You would have only noticed it if you were looking for it or if you were a parent, because that’s what parents do. After meeting with a pediatric orthopedic surgeon who specialized in scoliosis we learned she had two hemi vertebras in a row (malformed wedge shaped discs) in her thoracic region creating a curve of about 37 degrees at that time. We learned at that appointment that she would need surgery eventually but for now we would just monitor her through x-rays every three to four months.
It’s also not uncommon for children with congenital scoliosis to have other abnormalities, particularly with the spinal cord itself and heart and kidney abnormalities. This is because when the spine is developing in a fetus that development happens at the same time as the heart and kidneys. So Nora was scheduled for a full spine and spinal cord MRI, and echocardiogram and a kidney ultrasound at seven months old. Thankfully she had no other abnormalities present.
By time Nora was a year old her curve had progressed to 58 degrees and we were at a point where we had to sit down with her surgeon and figure out what to do next. Congenital Scoliosis is tricky.
Technically it is not a subset of early onset scoliosis subset but rather its own category. This is because the age of onset is prenatal and not between 0 and 5 which is how typical Early Onset is described. Congenital scoliosis is rare, occurring in only one of every 30,000 births. Spinal deformities in these patients have different treatments and prognoses based on the severity of deformation of the bone or bones, the pattern of deformity and whether the abnormal bones become more deformed as the child grows. There is limited research and studies regarding treatment of congenital scoliosis and therefore a lot of different opinions regarding treatment as well.
We wanted to pursue any options we had that were less invasive as surgery. It was our understanding that bracing very rarely works in congenital cases but metha/EDF casts can be successful. So when Nora was 14 months old we began the process of Mehta casting. We didn’t know if it would work, but our surgeon was hopeful. The goals of casting a child with congenital scoliosis are very different from those with idiopathic scoliosis. With idiopathic the goal is curve correction through a growth guided cast. In congenital scoliosis casting is used to buy valuable growth time before starting down the road of surgery. We aren’t looking for correction to happen; we are just hoping to slow the curve progression down that naturally happens during growth.
Casting children with congenital scoliosis is controversial and many pediatric orthopedic surgeons simply do not cast. Because congenital scoliosis is complex casting might not even be an option depending on the deformity and where. We were willing to try and see as the alternative was to just sit back and watch it progress and force into doing surgery sooner than anyone would want.
In the course of a year, we have been through five casts and we are happy to say her curve has held pretty steady and only worsened a degree or two. We are incredibly grateful we had a surgeon who was willing to take this approach and see if it would work. Nora is over two years old now and will soon be getting her sixth cast. We know surgery and/or surgeries are in her future and that’s another complicated road ahead of us but for now we are just gonna keep on casting as long as we can. It can work!
We are from a small Midwest town in KS and before the arrival of my 3rd beautiful baby girl on new years eve, 2003, I confess I had never even heard of infantile scoliosis. Utterly uninformed and ill prepared, I had no inkling that within a years time, not only would I have become fluent in the medical terminology, but I would also learn through many slammed doors that this diagnosis can also carry with it a death sentence.
Eliana Jeanne was born at 30 weeks gestation due to my out of control eclampsia/HELLP syndrome and underlying issues. With a birth weight of 2 lbs. 12 oz, she had experienced growth restriction and was tiny for 30 weeks. In spite of the steroid injection for her lungs before birth, they were still seriously under developed and that coupled with a diagnosis of both annular pancreas requiring high risk duodenum resegmentation within 24 hours and an atrial septal defect in her heart, we weren’t given lots of reason to be hopeful. As I nearly simultaneaously met my daughter, I was trying to kiss the air around her hard enough to say goodbye should that be the last time I saw her beautiful tiny pink face. She was given a 15% chance of surviving surgery and coupled with the mounting complications of prematurity, we were given a grim prognosis. Complications of a noscommial strep B infection through her cvc line and a left germinal matrix brain hemorrhage were just two of the life threatening challenges she faced. Over the course of the next 3 long months in the NICU, she battled her way back from deaths door more than once and I became forever changed by the tenacity of spirit I witnessed daily in such a tiny fragile vessel.
Interestingly enough her spine was however…never an issue. Spina bifida oculta ruled out, although there was present evidence of a small sinus dermal tract to her tailbone. It was closed and her spine was perfect. Proven over and over while keeping a close eye upon her lungs. Her perfectly straight spine apparent, week after week in the the chest films taken to warn of pneumonia or scaring. Finally at 3 months old, we took our very tiny miracle, heart monitor and all, home. Thriving now, all things felt possible given enough time, and our lives fell into one of predictable routine. In the weeks preparing for her 6 mo. well baby check, we began growing increasingly concerned about a slightly perceptible shift in her chest wall in the roundness of our grasp…and the fact she always slumped to the left unless being held. After passing her check up with flying colors, her doctor assured me that I was seeing issues out of fear and that I needed to accept that she was healthy now. I politely stated that I would do so as soon as I saw a chest film, and they needed to accept I had no intention of leaving without one. The look on the man’s pale face after returning with her films is one ill never forget, as it would become a repeating vignette over the next 6 months. We were looking at a right thoracic curve with a 55 degree cobb angle, 30 degrees of kyphosis and severe rotation in a spine that had been perfectly straight a mere 3 months prior. In 30 yrs of practice he’d never seen it before, nor did he know how to help us. He did however promise to help us find someone who did, and with that began our Scoliosis journey.
Starting at the closest major city, MRI films in hand, we began ping ponging around in an ever expanding circle of specialists. By our 3rd apointment we were given a traction suit of velcro & straps to derotate her spine, but did nothing except made her uncomfortable. Wait and see they said. More hopeful for our 4th opinion, we forged ahead to that of a highly acclaimed surgeon in St. Louis when she was 10 months old. She barely weighed 11 lbs and by this point had progressed to a lethal 100 degrees with 60 of kyphosis. No congenital reasons, no malformations, hemi vertebrae or underlying diagnosis. Idiopathic and a complete mystery, yet deemed the most severe in its nature. All that was certain was that in conjunction with her underlying lung and heart complications from birth, we were running out of time, so quickly my mind balked at taking its measure. “Wait and see” had become the only option given us due to her size but it was clear now however with her rotation deemed relentless that waiting had never been a viable option. Out of desperation at home we were using a modified gait walker to literally hang her from just below the arms in ‘traction’ several times a day and I had begun doing my own research. It was when “bring her back in 6 months, lets wait and see” was repeated by this renound surgeon, that I first uttered the word casting to this Dr.
True, I admitted, I knew nothing about it, but I was certain what more time would bring and I was willing to try anything at this point. It was also then that his demeanor shifted to one decidedly more curt and his response left me deflated and hopeless. Surgical intervention was not possible due to her small size and severity. I needed to come to terms with it, take her home and keep her comfortable. “Enjoy her while I had her, and we would see where we were in 6 months”. I knew where my baby would be in six months and it made me reel with anger. In disbelief that he was actually just giving up, I again pressed the topic of casting. This time he was entirely dismissive, called it barbaric and questioned what sort of parent would put their child through that. When I stated there was no need for another appointment in 6 months because I deemed waiting & watching her die ‘barbaric’, and that we would be seeking another opinion, he abruptly stood to leave and with the parting statement, “another opinion will probably only confuse you, but of course that is your prerogative” …he disappeared from the room…and so did we, never to look back. I want to be clear at this point that I am in no way disparaging the hospital in St. Louis, or even this Dr. Merely stating that in 2003, there was vast ignorance regarding the effectiveness of this treatment. In an ironic twist, I later saw this very surgeon that had given us no hope, years later in another panel of specialists there in SLC to learn. I wonder sometimes if it was Elianas updated presentation or her face that struck a chord to his memory…because on that day in the shriners lobby, he was silent but stared long and hard. You see, I had sent him a letter a couple years prior with a picture of Eliana at an age he said she’d never attain with a mere reminder that the option he’d dismissed as barbaric and old school, had managed to do what the surgical approach could not, and humbly asked him to keep an open mind. I was happy to see by his presence that maybe he did.
Far more compassion came from our next appointment in Denver, but sadly, no difference of opinion. 12 months old now and 110 degrees, sleep was fitful at best every night. The evening after our 5 th opinion, in my despair I stumbled across a parent support group online called I.S.O.P. The next morning after being granted access to this group…I finally gasped my first decent breath in months as I began pouring over the data in the links provided on the sight. Information about Dr. Min H. Mehta and her serial casting approach as a means to in some, cure, but in others, to buy precious time to grow. It was the first ray of hope afforded us since this had all started and I immersed myself in it into the early morning. Through the guidance and wisdom of the sites founder, Heather Hyatt Montoya, and her own incredible journey to help her daughter…the links to data published in Europe along with the support of parents on the site who helped narrow my focus, I settled upon the Shriners Hospital in Salt Lake City, Utah. Casting was available there and although retired, Dr. Min Mehta herself was traveling there for the very first Early Treatment Trial Project, showcasing her 40 years of data and bringing her style to the interested Dr.s here in the states. Eliana recieved her first cast at 13 mo old, in early stage cardiac failure from the pressure of her own tiny spine. Although her first cast was not a Mehta style e.d.f. cast (the first E.T.T.P was a couple months away) it saved her life and I attended that life changing conference with my once again thriving and growing baby girl.Every subsequent cast, starting with #2, through #33 which she is wearing now, nearly 10 years later, have been Mehta’s style growth guidance casts that have saved her life & become part of us now.
At 13 months, 115 degrees, 80 kyphosis and early stage cardiac failure… Eliana received her first cast with scaresly a second left to spare. We managed to harness one precious year of rapid infancy type growth before the rigidity of her curves made it become obvious that casting might not be a cure for us, but it has without a doubt become the one and only life saving tool with which we bought my daughter precious time to get to where she is now. Happy, healthy, beautiful, nearly 11 year old girl who is now big enough to embark upon the next step in her journey. We begin halo gravity traction in about 3 weeks in our hospital home away from home, and then on to growth rod surgery. A new approach brought to fruition within the last couple years, invented during this precious time the casts have purchased us.
I sobbed the first time I shook Dr. Mehta’s hand at that first ETTP, in awe of all that I’d been so lucky to find. It was a lifesaving miracle and I will forever owe Min Mehta’s research, our Doctors willingness and I.S.O.P’s assistance, an impossible debt. To that end is why I write this. I owe it to them and to every parent out there who has sat, blinking back tears at a computer screen desperate to find something that can at the very least offer a modicum of time. There is much more acceptance of this treatment now than the beginning of our journey thanks in large part to I.S.O.P. However as is true of all things in this age of information, there is much mis-information out there as well and sadly many children are still falling through the cracks. Its become increasingly clear to me how paramount getting out the accurate information is becoming.
I must state for the sake of that accuracy, and honesty, it was a very difficult thing to go through, that first cast. In spite of the fact it saved her life I still caught myself wondering as she cried nearly inconsolably upon first waking, “my God what have I done?” I thought it for hours as she barely ate and as I floundered at attempt upon attempt to get her diaper on, as she lie there already soaked in pee up her back within hours of what was meant to be a 3 month cast. Once the tears from the procedure subsided, the tears of frustration kicked in from it taking her newly acquired ability to crawl the first couple days, and now I cried openly with her. With each day however we both grew stronger and more accustom. She quickly learned to crawl again, and I how to care for the diapering and cast. She even learned to walk, all the while in a cast…and a small bike helmet for good measure, (we had hardwood floors). Each successive casting grew more manageable as we both learned what to expect…and the bounce back time has shortened after each and every cast since. She is now nearly 11 years old…and in her 33rd cast. Braces, although effective for some, don’t hold her rotation and at this point, stabilization is what we’re cultivating. Casting will not be a cure for my girl, but it has purchased us precious time to grow, and run and laugh and live a remarkably normal childhood. Thanks to casting, again like when I first brought her home, all things seem possible, given enough time.
Its why I feel compelled to say, don’t ever give up in pursuit of another opinion if your not being heard. Don’t believe every casting approach is the same, they are not. Pursue the data, the lions share of which came from the lifelong devotion and research of Dr. Min H. Mehta and has been made available through I.S.O.P. Don’t believe it if your told this approach is the old way or that its barbaric, it is not. Don’t accept “wait and see” in a curve you see with an increasing RVAD, the first couple of years when most flexible is time you cannot get back. We learned the hard way. Try to not get too caught up in the numbers. Its a marathon, not a sprint. More than that though, she’s absolutely thriving! Growing and attending school with her peers. Its true, impatience has lead me to other research just as I am certain we all have at some point…but it all leads to one inescapable truth. If I could leave you with one final thought it would be of that truth. Once instrumentation is introduced into the body the odds of complication are nearly 100%. If you think there is even the potential for this gentle, non invasive approach to help your young child…I implore you to empower yourself.
In the early 1940s, Dr. Harold Abramson, a New York pediatrician, pored over heartrending reports of babies who accidentally suffocated while they slept. As he reviewed case after case, he noticed that a vast majority of the deaths occurred when babies slept on their stomachs. After decades of additional research the federal government, the American Academy of Pediatrics and child advocacy groups formally launched the Back to Sleep campaign, instructing parents to place infants on their backs for sleep for the first year. There’s no question the Back to Sleep campaign has helped save lives. Since 1994 the rate of Sudden Infant Death Syndrome (SIDS) has declined by more than 50 percent. What this campaign has also effectively done is scare new parents so much that they don’t want to put their babies on their tummies ever.
More research suggests taking away “tummy time,” cuts off a pivotal avenue of development. The less time infants spend on their stomachs, the slower they generally are to acquire motor skills during their first year, which means the potential delay of simple feats like lifting their heads as well as more-complicated movements like rolling over, crawling, and pulling to stand. Doctors have hesitated to sound the alarm about this, since children usually walk shortly after their first birthday regardless of how much tummy time they’ve had. But a growing body of evidence now suggests that the timing of the motor-skill milestones that precede walking is crucial and can even factor into long-term health and cognitive ability. Pediatricians however, have had mixed reactions to this and have passed this off as inconsequential. Others, including the American Academy of Pediatrics, champion of the Back to Sleep campaign, have seen the head shapes and motor hang-ups as a harbinger of future problems and recommended supervised tummy time when a baby is awake.
Here’s where infantile scoliosis fits in. Parents are seeing the potential of death as outweighing the potential of delayed motor skills. What parents aren’t hearing are the increased risks of Infantile Scoliosis, the most challenging orthopedic condition in babies, from not having sufficient tummy time.
Prior to the 1980s the incidence of infantile scoliosis was much higher in Europe where infants were commonly placed on their backs to sleep. During this time babies in the US were traditionally placed on their stomachs to sleep and the incidence of infantile scoliosis was a rare phenomenon in North America accounting for less than .5% of all diagnosed cases of scoliosis. During the 1980s Europeans adopted the tummy sleeping position for children and the incidence of infantile scoliosis dropped to record low numbers.
Now take a look at Scotland before the 80s, where parents were routinely advised to place their infants to sleep on their backs, cases of infantile scoliosis accounted for 41% of all diagnosed scoliosis cases. After 1980 Scotland reversed their stance on back sleeping and the incidence of infantile scoliosis in Scotland dropped to 4%. At the same time there is research going as far back as 1966 that states one of the benefits of stomach sleeping was the prevention of scoliosis.
So what do parents do with this conflicting information? Putting an infant to sleep on his or her back is without a doubt the recommended sleep position for a baby’s first year of life. However tummy time is equally important and recommended for motor skill development and the prevention of scoliosis. The key is getting a sufficient amount of tummy time in. Parents should be encouraged to have their babies spend a healthy chunk of awake time on their tummies. This should begin soon after birth once the umbilical cord stump has fallen off. Several times a day so the child becomes used to it early on and likes it. There are lots of ways parents can practice tummy time, propping a baby on a nursing pillow while on the floor with them or even on a parent’s chest are great ways to get that added tummy time in and keeping everyone comfortable. Baby wearing is also greatly encouraged, as it too also helps promote physical development and decreases the risks of a baby developing infantile scoliosis. When parents choose a baby carrier it’s important to look for one that is comfortable to wear but is also ergonomic for baby.
Moriah was born by C-section at Via Christi St. Francis Hospital in Wichita, Kansas, on November 6, 1996. The next morning during her checkup, the doctor heard an abnormal heart sound and called in a pediatric cardiologist to consult. Moriah was diagnosed with Tetrology of Fallot, a congenital heart defect and she was immediately transferred to the NICU for observation. We were told that Moriah would need either a heart catheter or surgery within 1-3 months. When Moriah was 4 days old, we were able to take her home. Ten days later at a cardiology checkup, we were informed that she needed surgery as soon as possible, and she was admitted the next day at Wesley Medical Center. Surgeons placed a Blaylock-Tussig shunt in her heart to re-direct blood flow to allow for better blood oxygenation. This procedure bought Moriah some time to gain weight and grow before a repair surgery.
On the same day of her first surgery, Moriah contracted Necrotizingenterocolitus (NEC). The doctors called it “dying of the colon” and explained that her tissue was being attacked by infection. The presenting symptom was the mottling of the skin. There were three possible outcomes of the infection: no damage, minimal damage requiring surgery to remove the dead part and reconnect healthy tissue, or death. Moriah was treated in the PICU with three powerful antibiotics for three weeks. She spent another week on a regular floor and transitioned to discharge. I stayed with her throughout the ordeal, learning as much as I could about her medical care. This included running a Kangaroo pump and inserting putting a nasal gastric tube (NG tube), which I was afraid to do because I didn’t want to hurt her. The nurse simply asked me “Do you want her to eat?” I replied, “yes”. She said, “Then put the tube down.” That was exactly the no-nonsense approach I needed to make me do it. Little did I know I would be learning how to change a tracheostomy tube in a few short years.
Moriah’s father, Travis, visited our baby daily before and after work. He whispered in her ear that she was doing a good job and encouraged her to keep fighting. He nicknamed her “mighty Mo” after the Mighty Missouri. Our family, friends, and church supplied nearly every meal for us during her month-long hospitilization. We are so thankful that there was no long-term damage done by the NEC. Moriah was fed through an NG tube for six months while we worked with therapists to maintain bottle feeding and eventually take in solid foods. Moriah also had physical and occupational therapy for a year to build up muscle tone lost from being immobile in the hospital, and to help her meet her developmental milestones.
During a cardiology checkup at about 3 months of age, chest x-rays showed a curve in Moriah’s spine. The cardiologist explained that congenital heart defects are often paired with another congential defect such as scoliosis. Moriah was referred to a local orthopedic doctor, who measured her thoracic curve at about 30 degrees. We were directed to wait and watch, with appointments every few months to see how the curve would progress. Travis inquired whether there were any type of cast or brace Moriah could wear to hinder the progression, and we were told there was not. The doctors were mainly focusing on resolving Moriah’s heart problems first, and did not want to restrict her chest cavity. We were not given any information on an RVAD measurement, or congential anomalies such as hemivertebrae.
At 7 months of age, Moriah had an MRI. Even then, we were not given any additional information or guidance beyond “wait and watch.” Years later, when we requested all of Moriah’s medical records, we found the report showed she did have at least two hemivertebrae at that time. By the time we had that knowledge, Moriah had undergone so much fusion that it was impossible to tell if the diagnosis had been correct. At the time of the initial diagnosis, my husband and I didn’t even know what questions to ask and we could find nothing on the internet to give us direction. We trusted the orthopedic doctor’s advice: we waited and watched Moriah’s scoliosis get progressively worse.
Moriah underwent her second open heart surgery to repair her Tetrology in April of 1998, at 17 months of age. This was our first surgery away from home and family. Thoracic surgeons at The Children’s Hospital (TCH) in Denver patched a hole to decrease the amount of mixing oxygenated and un-oxygenated blood, and they widened an artery. Moriah was sent home on a low dose of oxygen. We learned how to administer oxygen and monitor her oxygen saturation rate via a “sat” monitor.
By November of 1998, at two years of age, Moriah’s scoliosis measured 90 degrees with rotation and kyphosis. Our orthopedic doctor referred us to an orthopedic surgeon who measured Moriah’s curve at 115 degrees and recommended spinal fusion to slow the progression. We trusted this advice, and Moriah had her first fusion surgery on November 19th, at Via Christi St. Francis. She wore a TLSO brace 9 months following this surgery. We asked the surgeon whether the brace would correct the scoliosis at all before the fusion set. His response was no, the brace was only to protect the fusion as it set over the next 6 months to one year. In August of 1999, we again traveled to Denver for a heart catheter and to check on the results of the Tetrology repair surgery.
Shortly before May 2000, we learned that Moriah’s fusion had not stopped her curve and that it was “crank shafting.” Moriah underwent a second spinal fusion surgery that month. She was now fused anterior and posterior. After this surgery, Moriah experienced difficulty breathing and needed C-pap and oxygen. She stayed in the hospital a little longer than normal, but went home without oxygen. Moriah again wore a TLSO brace for 6 months. Her little brother Declan was born October of 2000.
During the winter of 2001, Moriah’s cardiologist informed us that a leaky valve in her heart had worsened and needed to be replaced. Moriah had become pale, lost energy, and her saturation levels were lower. Because performing the necessary operation during the winter would risk pneumonia, Moriah was scheduled for surgery in Denver in April. When we arrived at the hospital, her surgery was postponed due to poor lung function. While her valve did need to be replaced, it was her restricted lungs that were causing the low oxygen saturation numbers, according to pulmonologists and TCH. My husband and I had been told by both Moriah’s cardiologist and orthopedic surgeon that Moriah would have “restrictive lung disease.” They explained that this was due to her weakened heart function, and that she would become “winded” more easily. This was the first time we understood that there was a connection between Moriah’s scoliosis and her lung function. Previously, our focus had been on getting her through the numerous surgeries and having as normal a life as possible in between. While in Denver, Moriah had a heart catheter and a stent placed in one of her arteries. Doctors considered whether or not Moriah needed a tracheostomyat that time to help her breathe. At her heart surgeon’s request, we also consulted with a pediatricorthopedic surgeon. We discussed options to address Moriah’s scoliosis, which was threatening the repairs to her heart. Upon dismissal, we were advised to see a pulmonologist as soon as we got home. Ironically, the specialist we were referred to was in the same building, on the same floor, one hall down from Moriah’s cardiologist. Moriah began bi-pap therapy at night to help her exhale fully, expelling more carbon dioxide. Two sleep studies were done to check the bi-pap settings. Moriah also had carbon dioxide level checks periodically.
December 2001 Moriah had the leaky valve in her heart replaced at TCH. She was hospitalized only 8 days and went home on a low dose of oxygen. While we were in Denver this time, her heart surgeon again asked us to consult with the same pediatric orthopedic surgeon. X-rays showed that Moriah’s curve was again moving despite the fusions. The heart surgeon was concerned that Moriah’s progressing scoliosis would cause damage to the repairs done on her heart. He was also confident that, once recovered from the most recent surgery, Moriah’s heart would be strong enough to withstand a major spinal operation. We decided to have Moriah undergo halo traction in a wheelchair in an effort to reduce her curve and take pressure off her heart and lungs. We were told they expected up to a 50% curve reduction.
In May of 2002, surgeons in Denver broke apart some of Moriah’s previous fusions, removed some of her growth plates, and put in new fusion. A halo was applied to her head with 8 pins to distribute the traction weight. This proved to be her most painful surgery experience. Moriah required heavy pain medication to withstand the first two weeks of traction in the wheelchair. It took two weeks to wean Moriah from the ventilator this time. When, after 3 days, her CO2 levels went back to the 70s, we agreed to a tracheostomy surgery. Moriah was not doing well on bi-pap and passing out in her wheelchair traction. She did not have any energy to eat and the NG tube could not be removed.
All totaled, Moriah and I spent a month in Denver this visit. Travis flew home two days after the spinal surgery to resume working, so this was our first hospital stay apart. We had daily cell phone updates. Our son, Declan, was 18 months old at the time, and he stayed with us in Denver for 3 weeks at the Ronald McDonald House. My friend, my sister, and my aunt and young cousin each took week-long shifts, flying out to Denver to babysit Declan. When we knew Moriah was going to have the tracheostomy we decided to send Declan with my aunt and cousin. He was with them for 5 weeks, away from his parents and sister. Every trip to the Denver airport made me cry as others went home and we were still in the hospital. We saw Travis once more before transferring via medical flight to Wesley in Wichita, Kansas: he surprised us by arriving the day of the tracheostomy surgery. Moriah had told me before they took her in that she wished Daddy could be there because he helps her to be brave. When she woke up from an evening nap, there he was, smiling at her.
Moriah spent 5 weeks in the PICU at Wesley. Travis again visited every morning and after work. I slept at Moriah’s beside or in a nearby parent sleep room. Family and friends showered us with food and things to occupy our time. Teen volunteers decorated Moriah’s room like we were having a party, to cheer her up. Moriah recovered slowly as we increased the traction weight. Moriah only weighed 27 pounds, and had never been able to gain much weight on her own. We asked the pediatric intensivist for an appetite enhancing medication, and he recommended Megesterol (Megace), a medication often used for patients who experience appetite and weight loss due to AIDS and cancer. It is also used with individuals who have difficulty gaining weight due to multiple surgeries. Moriah was started on Megace, and resumed physical and occupational therapy to fight against muscle loss while in the wheelchair. She worked to be able to use the restroom out of traction with someone holding tension on the halo.
As a parent of a child with a trach, I learned to change and clean the trach tube. I also learned suctioning, manual chest percussion therapy (CPT), cleaning of the halo pin sites, and Moriah’s physical therapy routine. Before we left Denver, the physical therapists made a video of how to transfer Moriah from her bed to the wheelchair, how to hold tension on the halo while she walked out of traction, and how to hook up the traction line and weights, both in the bed and the wheelchair. I shared this video with the nurses and doctors at Wesley, as they had not worked with this type of traction before. Moriah was discharged from Wesley on a ventilator. Before we were allowed to take her home, in-home nursing staff was set up. My husband and I also had to demonstrate that we were capable of caring for Moriah on our own for a number of hours a day. This included understanding her vent settings, and what to do or who to call if complications arose. We turned one room of our house into a psuedo-hospital room. We isolated the wiring to its own breaker, had a medical bed delivered, set up organized space for supplies. We also had an oxygen concentrator, backup O2 for power outages, an external backup battery for the vent, a portable suction machine, and an O2 sat monitor. Moriah was also sent home with the NG tube, so we had the Kangaroo pump again. Our home nurses were used for pin-site care and trach-care, but were unfamiliar with Moriah’s traction. I had them watch the video and showed them what I had been taught.
The experience of having nurses in our home has been both comforting and stressful. We really have to be aware of having family time. The trach made it necessary for our home to be open to nurses, respiratory therapists, and their case managers. We also, for the first time, had to apply for Medicaid to cover Moriah’s increasing medical expenses. While it is great to have Medicaid pay for what insurance will not, the financial limits the system forced us to follow to retain coverage were unreasonable. Our family was used to being independent, and it was very hard to ask for help. No one, no matter their earnings, can afford the costs of the medical equipment rental and nursing. Yet, without those things in the home, Moriah would have spent her entire traction time in the hospital. Kid-Screen, a case management program offered in Kansas, fought several months to have Moriah placed on the TA (technology assisted) Waiver list. With this classification, Medicaid no longer scrutinized my husband’s wages, and we no longer feared losing our home while trying to earn under their limits.
Moriah was in halo wheelchair traction for a total of 7 months. X-rays were done monthly at Wichita Clinic with a local orthopedic doctor who emailed them to Moriah’s surgeon in Denver. During this time Moriah rode the wheelchair bus to kindergarten. Since the school did not have a full-time nurse to watch over Moriah, one of our home nurses attended school with her. The orthotist who made Moriah’s two previous TLSO braces furnished us with an “off the shelf” neck collar to wear on the bus. He enlarged an opening so her trach and ventilator tubing wouldn’t be disturbed. Moriah remained on the vent and eventually weaned to a Passy-Muir valve during the day. We put her T-bird vent, suction machine, O2 Sat machine, oxygen tank, and medical supply bag in a Radio Flyer wagon and pulled it behind the wheelchair everywhere Moriah went. By December, we were up to 25 lbs. of traction weight and Moriah’s scoliosis had reduced to approximately 60 degrees. She had gained 5 inches in height and 16 pounds in weight.
December 13, 2002, the halo was removed in the surgeon’s clinic in Denver. We had not been advised that this could turn into an overnight procedure involving anesthetic, and we had not planned for that in our trip. The surgeon said it would be alright to remove the halo in the clinic if Moriah could hold still enough. We had also not been told that traction weight should be removed as gradually as it was added, so Moriah went from 25 pounds of traction weight to nothing in a matter of minutes. She was so brave and still as they loosened each pin and pulled them out. When they told her it was safe to move, she lunged into my arms, crying. Although my husband and I asked, a brace was not recommended, nor was physical therapy prescribed. Moriah was in a great deal of pain without the traction support. We obtained orders for Lortab and physical therapy from our family doctor at home.
Just a few months later, in March 2003, we noticed that Moriah’s kyphosis looked worse. X-rays showed her curve had increased to 80 degrees. We contacted her surgeon, who explained that it was a “settling” effect from being out of the traction. We again asked for a brace to stabilize this “settling” and were told Moriah did not need one. By November 2003 Moriah’s scoliotic curve had reached 120 degrees with 120 degrees kyphosis and rotation.
About this time, we learned of the Vertical Expandable Titanium Rib Project (VEPTR) through the Infantile Scoliosis Outreach Program, and initiated contact with the University of Texas Health Sciences Center, in San Antonio, Texas, where the new procedure was being performed. In January of 2004, Moriah was rejected for the VEPTR implants because of the severity of her kyphosis.
February 2004 we took Moriah to Denver for a 3D CT scan. Both her scoliosis and kyphosis measured in excess of 120 degrees–almost immeasurable due to the rotation. The CT scan showed cracks in her fusion at T8 and T11. We later found documentation (referred to earlier) stating that Moriah had hemivertebrae at T9 and T10. After weighing options, we chose to repeat the halo traction process and to have as much of her previous fusion as possible removed. We were told that this should be her last halo in light of scar tissue, etc., and we wanted her spine to be as flexible as possible. The surgery could not be scheduled until May, and the surgeon did not feel her spine could get much worse in the meanwhile.
In May of 2004, Moriah underwent 9 hours of surgery. The surgeons were not able to release as much fusion as they did in the previous surgery. Nor did they have an optimistic prognosis for correction: possible only to 90 degrees instead of the 60 degrees we were hoping for. Also during this operation, her thoracic surgeon, who was assisting in the approach, noticed two portions of diseased lung tissue, the size of fifty-cent pieces, on the lower lobe of the left lung. He removed the diseased tissue as it was “an infection waiting to happen.” Because Moriah’s spine was so close to her ribs, they cut the ribs apart to gain access to the fusion, and then wired them back together. Thankfully, Moriah experienced no nerve loss in that area. Some of the complications Moriah experienced from this surgery included: pneumonia, UTI, bladder retention, and clonis in her ankles. They put her on a cuffed trach with an inner bubble that blocked all air leaks, preventing her from speaking for over a week. This took a toll on Moriah’s usually cheery disposition.
While at TCH, I initiated discussions with the orthopedic department about constructing a traction walker from a photograph of one used at the Shriners Hospital in Utah. TCH orthopedics were willing to try if a walker could be found, and if the funding were approved for the extra traction tubing needed. The walker would cost $600 and was not in the hospital’s budget. A great friend of ours posted an email on Parent to Parent of Colorado explaining Moriah’s need for a specific type of walker. Within 8 hours of the post, a parent was at the hospital donating the exact walker needed.
Moriah was once again transferred to Wesley via air ambulance to complete her recovery. The walker was not yet complete, and the wheelchair wouldn’t fit on the plane, so we had to leave Denver without them. We were able to get a pediatric wheelchair from a medical supply company. While at Wesley, we waited for her home ventilator and backup vent to be shipped from California. The model we were to use was new to the Midwest. Moriah continued physical therapy and her clonis improved. Two weeks later, when Moriah was discharged from Wesley June 7th, the walker was still being built in Denver. Moriah began to experience weakened leg muscles and her knee locked uncontrollably when she was out of traction, walking to the restroom. Through the efforts of Lynx Collaborative Care Network, the walker was delivered to our home on the July 4th weekend. Lynx paid the travel expenses and hotel so the person who built the walker could deliver it and show us how to use it properly. The walker was the best thing for Moriah. She became stronger, and the clonis, weak leg muscles, and knee locking stopped. Mentally and emotionally, Moriah benefited from being able to walk around most anywhere. She attended second grade with the walker, feeling independent, and more like the other kids. She was also able to participate in more adapted activities in P.E. and at recess.
In addition to their assistance with the walker, Lynx executed the overwhelming task of compiling Moriah’s medical documentation from all the offices and hospitals where she had received care. They also sent an informative and concise update on Moriah’s progress to San Antonio for reassessment for the VEPTR implants: Moriah’s scoliosis had reduced from 120 degrees to 65 degrees and her kyphosis had reduced from 120 degrees to 72 degrees, making her a more viable candidate for VEPTR. The day before Thanksgiving in 2004, we learned that Moriah had been accepted to receive the implants.
February 16, 2005, Moriah received two rib implants on her right side. The Family Medical Leave Act allowed Travis to take 3 weeks without pay from work, and we spent our tax refund to cover our bills so we could all be together in Texas. The implant surgery lasted 4 hours with no complications. Moriah’s recovery was quick due to great pain management, and no postoperative infections or complications. She was hospitalized only 2 weeks. All of the doctors, nurses, and respiratory and physical therapists were wonderful. We will return to San Antonio July 26th for Moriah’s second VEPTR implant surgery. She will have a single VEPTR placed on her left side. They will also move up the anchoring point of one or both of the VEPTRs on her right with the hope of better addressing her kyphosis.
We are so grateful to Doctors Campbell and Smith for inventing the VEPTR device. We would not be this far in Moriah’s treatment without the Infantile Scoliosis Outreach Program and Lynx Collaborative Care Network of Colorado. And we would not be sane without the unending support of our family, friends, church, home nurses, and community. Moriah is excited to be going on to third grade, and will have her same nurse there at her side until her trach can be taken out permanently.
There is too much as yet unknown about infantile scoliosis. It is unacceptable to “wait and watch” children like Moriah get worse. Research is a parent’s best tool in understanding scoliosis and working together with the doctors to chose the best treatment plan for their child. Moriah is a very strong girl and we have made a point of explaining to her, to the best of her understanding, every step taken to pursue her health. We teach her that while “medical stuff” involves a great part of her life, it is not her whole life. She can be and do anything she sets her mind to. It is our hope that, by reading Moriah’s story, you will learn from our mistakes, smile at Moriah’s progress, and be inspired to diligence in seeking the best care for your child. Make your list of regrets as short as possible.
Moriah is almost 10 now and enjoying 4th grade. In July 2005 she had one VEPTR hybrid placed on her left side. In February 2006 her surgeons re-seated the upper anchor on her right side to better address her kyphosis. They also switched out the lower anchor at that time converting it into a hybrid. Moriah now has one hybrid on each side and one cradle to cradle VEPTR on her outer right side. July 2006 was Moriah’s first expansion only surgery. It went better than we could have hoped. She was ready to go home the very next day. We have had zero complications with Moriah’s VEPTR implants. She will continue to receive expansions of her implants every six months until she is between the ages of 14-16.
Moriah’s lung health has improved dramatically. She is now off the ventilator completely. Moriah has her trach capped 15hrs a day and uses oxygen at night. Her pulmonologist is so pleased with the improvement that very soon Moriah will be capped 24 hrs a day. If she has a good winter, we have hope that the trach will come out in the late Spring or early Summer 2007. Routine bronchoscopies have documented the changes in Moriah’s airway. It is now strong, not floppy, and her bronchi openings are nearly symmetrical, all due to a decrease in Moriah’s scoliotic curve. She also recently had a complete heart exam during a catheterization that showed no signs of complications. We are so excited to be on the other side of all the struggles these last several years.
Update on Moriah April 2007
Moriah had her second, expansion only, surgery Tuesday, March 27th. Everything continues to go well with her VEPTR implants. On March 13th, Moriah regained freedom she hasn’t had in 5 years! Her trach being no longer necessary, Moriah took it out herself, under doctor’s supervision at the hospital. She was able to finish 4th grade without the supervision of a nurse going with her to school.
After 8 weeks the stoma had only partially closed. An ENT closed it for her surgically May 29th. After 10 years of struggle, Moriah is finally at a maintenance point with her scoliosis, heart, and lung issues. We will continue to vigilantly monitor her heart, lung and scoliosis as she grows. We could not have come this far without our ISOP family. This organization and the families involved are truly a blessing from God!
Update: September 2007
We were in Texas once again in August for expansions. Everything went perfectly. Moriah and I were invited to a Q & A session at The University of Texas Health Sciences Center at San Antonio. Dr. Simmons spoke before the new medical students in their Gross Anatomy class. Afterwards they asked Moriah and two other panelists questions. She did a great job! We put in a good word for ISOP! Moriah is in the 5th grade this year! She shocked us all by deciding to play the trumpet. What a great thing to get her involved with her classmates. Her doctors are happy about how it will improve her lungs! It is truly wonderful to see her so healthy. We’ve waited a long time for this and feel very blessed.
Halo gravity traction is a procedure used to reduce the degree of curvature in the spines of children with severe idiopathic or congenital scoliosis. Spinal traction is the gentle pulling of the soft tissue (joints and muscles) to help straighten the spine. A scoliotic curve allowed to reach high degrees of measurement may increase pressure on the lungs and heart. The result can be a decrease in life expectancy by up to twenty years.
Who Needs Halo Gravity Traction?
Halo gravity traction is needed by children with severe curves in their spine (80+degrees) who have not had success with other measures of correction, such as serial corrective plaster casting and serial bracing. Halo traction is also needed by those children with high curves who are not eligible for other measures of correction because of congenital defects in their spines. Many of these children are already experiencing stress to their heart and lung functions. Patients with severe infantile, juvenile and adolescent scoliosis and Scheuerman’s Kyphosis may be considered likely candidates for halo traction.
What is the Expected Outcome of Halo Gravity Traction?
Each child with severe infantile scoliosis will experience a unique outcome. Many factors, such as the stiffness or flexibility of the spine and whether congenital scoliosis with previous fusion is present, will affect the outcome. The goal of treatment is to safely bring the curve to the smallest possible degree and delay spinal fusion (if not already fused) until spine growth is close to finished, or maintain correction achieved via serial casting, bracing or instrumentation. Typically, a curve is reduced by about 50%-60%. The emphasis is placed on the child’s heart and lung health and not the number of degrees.
Application of Halo Gravity Traction
While the child is under general anesthesia, a horseshoe shaped metal bar is secured to the skull with 4-8 pins. These pins distribute the traction weight evenly. The number of pins used is in relation to the child’s weight. The halo will sit slightly above the eyebrows and reach back to the child’s ears. In some cases, it can go completely around the child’s head. The pins will hold the halo in place a short distance from the forehead. Once the halo is secured, it is ready to accept the traction weight. Traction is achieved by weights hung from a rope woven through a precise pulley system to the triangle and carabineer attached to the top of the halo.The traction gently pulls against the child’s body weight to straighten the spine.
The amount of traction weight used is determined by the orthopedic surgeon and depends on the child’s body weight (approximately 1/3 of the child’s weight).Traction weight starts light and increases slowly and deliberately until the maximum traction weight for the particular child is reached.
Halo in Place
The traction weight is decreased at the same deliberate pace, working towards the goal of halo removal, once correction is obtained.Following the placement of the halo, the child will remain in traction at all times. The apparatus
for traction is made to fit the bed. Maximum use of gravity is obtained by placing the bed in the Reverse Trendelenberg position, a downward slant of the bed where the child‘s head is elevated and feet are lowered. Newer beds have motorized controls to accomplish this. On older beds a stabilizing block can be constructed (see article) and resume physical activities. Maintaining strength while in the halo is very important so the child can return to normal activities when the halo is removed.
Your child’s orthopedic surgeon will determine whether your child will achieve more correction if wearing a cast during the halo procedure. Children who are scheduled to undergo a VEPTR implant surgery may not require plaster casting during the halo procedure, due to the necessity of maintaining healthy skin pre-surgery.
Possible Complications and Monitoring
Some possible complications from halo traction are: pain and weakness in the neck muscles, swallowing muscles and tongue, pain and weakness in the eyes, infections at the pin sites and neuromuscular complications. These are rare due to strict monitoring of thechild’s neurological functions through simple tests of the eyes, facial muscles and movement in the arms, legs, toes, etc. Caregivers will be taught how to keep pin sites clean, and nursing staff will monitor the appearance of the skin around the pin sites daily. Check with your child’s orthopedic surgeon to see if physical therapy might benefit your child during this process. Any cause for concern should be discussed with your doctor immediately.
Pursuing Halo Traction Treatment
Each hospital equipped to provide halo traction treatment will have specific protocols for patient acceptance for the procedure. The following is a general outline of what you might expect:
Undergo an assessment by your pediatric orthopedic surgeon and be identified as a candidate for halo traction treatment.
Meet with your surgeon to review what halo traction is, its purpose, and the intended outcome for your child.
Meet with the anesthesiologist to discuss sedation methods and any allergies your child has had to anesthesia or medication in the past.
Meet with the pulmonary department to discuss whether or not there is a need for Chest Percussive Therapy (CPT) or other breathing therapies such as Bi-Pap.
Meet with physicians to discuss pain management. Many hospitals have a pain team that will discuss with you the various pediatric medications used and their side effects.
Review teaching material on patient preparation and patient care.
Tour the orthopedic floor of the hospital and see an example of the traction apparatus mounted to a bed, wheelchair or walker. See examples of the casts and braces used.
See photos of other kids in halo traction to prepare yourself for what your child will look like. Immediately after application, your child’s head may be bruised, red, swollen, and there may be drainage from the pin sites until they have healed.
Share your child’s health history and medical portfolio with the orthopedic surgeon and his team, so unnecessary x-rays and tests are not repeated.
Pursue an assessment by the physical therapy department to determine your child’s pre-traction capabilities and strength.
Meet with hospital social work staff to discuss psychological implications of being hospitalized for up to three months. Discuss the importance of an emotional support system, and their involvement in helping you and your child maintain a positive outlook and successfully complete the long stay in the hospital. Discuss services that may be available to your family within the hospital, such as referral to hotels offering a medical rate and discounted vouchers for meals in the hospital cafeteria.
Meet with child life specialists to discuss activities to divert your child, educational services available for school age children, and tour the playroom, movie check-out closet, library, etc. Many hospitals have scheduled activities for the children and Pet Pal programs, where specially trained dogs visit the children.
Preparing the Family for the Halo Gravity Traction Procedure
A caregiver should plan to stay with the child at all times. Your child could be in the hospital for 8 -12 weeks, depending on the severity of the curve, your child’s overall health and strength, and the intended outcome for your child determined by you and your surgeon. Halo traction is meant to be a gradual process to limit overstressing your child’s body.
Your child will need help daily with personal care, toileting, eating, transferring in and out of bed, transferring from the wheelchair and walker, pin care and physical therapy. Be willing to learn how to care for your child. Communicate with doctors and nurses regarding your feelings about participating in your child’s care. Practice transferring your child before the halo application. Also practice holding the weights and traction to prevent injury.
Your child will also need emotional support and encouragement. Children will react to being away from home. They will react to having their movements changed and restricted. They will react to the pain felt during the first week of traction. Some children will not want to see themselves in a mirror or a photograph. How you respond to your child will largely shape his or her attitude toward the traction process. The first and last weeks of traction are typically the hardest. The caregiver staying at the hospital should prepare to support the child through these difficult times. The support of family and friends during this time helps tremendously. Friends and family can provide special meals, presents and cards to cheer the child, or maybe even sit with your child so the caregiver can take a break. Have someone outside of the situation that you can talk to about your feelings without upsetting your child.
Parent sleeping rooms, showering facilities and laundry facilities are available in many hospitals. Many hospitals are also near hotels that offer a medical rate and charitable housing, such as the Ronald McDonald House.
Plan to bring some of your child’s favorite things to decorate his/her room. A favorite blanket or stuffed animal, music CDs and movies are helpful also.
Preparing the Child for Halo Traction At Home
Seeing pictures beforehand of other children in halos may be helpful. If possible, talk with other families who have gone through the process. Encourage your child to ask questions and make sure those questions are answered. Make sure your child understands the necessity and purpose of the halo traction procedure. Emphasize the fact that the treatment is a short-term hindrance or frustration compared to the lifetime affect it will have on their health and the degree of their scoliosis.
In the Hospital
Clothing: Your child will be most comfortable in loose fitting clothing. Button-down tops work best. If your child is in a cast, elastic pants are recommended.
Bathing: When bathing, only baby shampoo should be used. The chemicals in other products can react with the metal used in the halo and pins.
Diet: Maintaining your child’s weight during traction is important. A regular diet may be resumed soon after surgery. Supplemental items may be used to add calories if needed. Because the traction limits movement of the head and neck, it will be necessary to encourage your child to take small bites and chew them well. Use a straw for drinking. Small, frequent meals that are nutritious and high in calories are best.
Sleeping: Your child will be in traction while sleeping. A rolled towel or small pillow can be used for head and neck support. An egg crate or foam pieces can be added to the hospital mattress for more comfort. The bed should also be tilted in Reverse Trendelenberg, so the head is higher than the feet. This adds the pull of gravity to the traction while your child is lying down.
Physically handling your child: At first your child may feel awkward and unsteady in the traction. Once he or she gets used to the traction, moving around will be easier. You will be helping your child move from a wheelchair, walker and bed. Nurses and physical therapists will help you learn which movements are safe for your child.
Pain management: Each child will experience pain in varying degrees. Medications are used to control your child’s pain. Good pain control is crucial to your child’s recovery from the halo application. Pain medication may also be used at night, so your child can sleep. Rest is important to maintain strength and a positive attitude. Your child’s pain should decrease over time. Discuss all pain medications and their side effects with your doctor. Many pain medications cause constipation. Laxatives, high fiber food and plenty of fluids help counteract this side effect. Never hesitate to communicate your concerns about your child’s recovery with his/her doctor. Communication with your child’s doctor is crucial in ensuring your child has a quick recovery.
When Halo Traction is Finished
When your orthopedic surgeon feels the intended outcome has been reached or that maximum correction has been achieved, the halo (and, in some cases, the cast) will be removed. If your child will be braced, a mold of your child’s body will be taken to make a brace. There are many different kinds of braces with many specific purposes.
After the brace is made, your child will wear it for approximately two weeks, while the traction weights are systematically decreased. Frequent brace adjustments may be needed based on the complexity of the brace.
Your child may experience some aching and discomfort during the weight decrease and transition into the brace. A slight loss in correction may also occur.
After the halo is removed, your child’s neck muscles will be weak and need support. A soft, removable neck collar is suggested to support those muscles until they are regained through physical therapy.
Before being released from the hospital, your child must feel comfortable in the brace. (Caregivers must also feel confident about taking care of their child while in the brace.)
Your physician will tell you how many hours per day the brace is to be worn. It is important that those instructions be followed to maintain the correction achieved through halo traction. Your physician will also inform you of how often to come in for follow up visits to check the fit of the brace and how the curve is maintaining. New braces will be made as your child grows. A brace should be worn as long as it is successful in maintaining your child’s improved scoliotic curve.
Brace Care
Caregivers should be taught how to properly put the brace on and take it off. Make sure you feel comfortable doing this before leaving the hospital.
Bathing and skin care: The brace may be removed for bathing. It is best to wash your child’s hair at this time as well. No lotions, creams or powders should be used on your child’s back. These items can irritate the skin. Alcohol can be wiped on your child’s skin to toughen it up and prevent itching, rashes, sores, pimples and smelly odors.
Clothing: Necklines may need to be larger to fit over the brace.
Diet: As with casts, food should be cut into small bites and well chewed, and straws used for drinking. The brace may also put pressure on the abdominal wall, so small, frequent, nutritious meals, high in calories are best. Some weight loss may be expected, and supplements can also be used to help your child maintain weight and strength.
Movement: Continue to follow the precautions you learned in the hospital for lifting your child and helping him/her sit up or get out of bed.
Exercise: Your child may require physical therapy or some type of respiratory therapy. Caregivers should be familiar with these exercises and how to perform them.
Note: This information is provided by the parents of children with infantile scoliosis to other parents, not by physicians. It is for general informational purposes only and cannot substitute for the advice of a medical professional. The information provided on this website should not be used for diagnosing or treating any medical condition. ISOP disclaims any responsibility whatsoever for the results or consequences of any attempt to use or adopt any of the information provided on this website. Nothing on the ISOP website should be construed as an attempt to provide a medical opinion or otherwise engage in the practice of medicine. Please consult your child’s physician for diagnosis, medical advice, and answers to your personal questions.
Rocco was born 10 days early in June 23, 2011. He had an exciting birth as he was born bum first (breech) with a room full of doctors and nurses that wanted to see his unusual birth. Thankfully he was healthy. We were over joyed to have our little boy and to bring him home to his big sister.
At his 8 week check up, I mentioned to his nurse practitioner that I thought Rocco’s right shoulder seemed higher then the other. She recommended that we see a physiotherapist. His physiotherapist then diagnosed Rocco with Tortacollis (a short neck muscle) that was causing his head to tilt to the one side and made it appear that his shoulder was higher. After weekly appointments and painful exercises we lengthened his neck muscle and his Tortacollis went away. He was 6 months old when his physiotherapist noticed that his back looked alittle crooked. He then sent us to a paediatrician. We have also seen 2 neurologist, a genetic specialist and a orthopaedic doctor. It was the doctor at McMaster Children’s Hospital in Hamilton, Ontario that gave me the shocking need of Scolocsis. I felt like the wind was knocked out of me. It was just me and my baby boy locked safely in his car seat and my mind was racing about what this meant for his future. I also had to give the diagnoses to my hubby. We then saw 3 different orthopaedic doctors, Rocco’s has had 5 X-rays and an MRI. He has consistently remained at about 55 degree curve and thankfully his MRI did not show any underlying condition.
We were told like so many other parents that we should wait and see and that Rocco would eventually may need to have surgery. We just could not settle with that fate for our boy.
After a lot of research and speaking to many wonderful parents on ISOP we decided to travel from Canada to Shriner’s Children’s Hospital in Erie Pennsylvania to begin his Mehta Casting. Rocco received his first cast on September 10, 2013. He was about COBB 58 RVAD 2. We are thrilled and so thankful to have found ISOP and Shriner’s. It was defiantly a difficult experience getting his first cast but the support from the families from ISOP and the staff at Shriner’s was invaluable. We felt like we had so much support that helped us get us through.
Rocco has settled with his new life in casts and has bounced back to being the happiest little guy. We have now had four casts and he is currently in a summer brace. We will continue casting this fall. His last numbers where out of cast 36.4 degree top curve and 31.3 degree bottom curve
When Alyssa was around a year old, my husband and I started noticing that her shoulders were a bit uneven, shoulder blade and rib cage protruded and her torso was slightly twisted. In the beginning we thought that maybe she was just “double jointed”. We mentioned this to the pediatrician at the time and her reply was ” she’ll outgrow it”. As we started noticing that it wasn’t getting any better and in fact seemed to be getting worse, we would attempt to mention it to the pediatrician and somehow the subject was avoided and immediately changed. It was until May 2012 ( 2 months before her 2nd birthday), that we as parents decided to seek a second opinion and took Alyssa to St. Christopher’s Hospital in Philadelphia. There we realized that she had scoliosis and the chances of her “outgrowing it” were slim to none. It was estimated that her spine was curved at approximately a 50 degree angle. As a parent, I felt my heart stop beating and an emptiness in my stomach. We were informed of the risks associated with scoliosis including but not limited to cardiac & pulmonary issues however at this point the orthopedic surgeon at St. Christopher’s wanted to “watch & wait” and see if and how it progressed. Needless to say without any treatment her spine continued to curve and our next MRI showed a curve of 67 degrees( January 2013). In the meantime, we went to visit with a cardiologist and determined that Alyssa had a small heart murmur but wasn’t anything too serious ( we would just watch and make sure it didn’t become compromised due to the curving spine). At this point, the orthopedic surgeon from St. Christopher’s referred us to Shriners in Philadelphia to meet the the doctors there. In April 2013, Alyssa had an MRI done which showed an 87 degree curve in her thoracic spine . The surgeon at Shriners introduced us to something called a “Mehta Cast” which is a plaster cast that Alyssa would be fitted for and would wear this cast for 10-12 weeks at a time with a small break in between. This was/is our best possible answer considering that surgery was out of the question due to her age & size.
Here she spent the night and we learned all about “Flossing & Petaling” the cast. As with any type of plaster type casts, this meant no more baths or pool time. Alyssa was scheduled to go back in to have the cast changed in early October when we were notified that a Chiari Malformation was detected on her MRI. We had her cast removed in early October and Alyssa went back to St. Christopher to meet with a neurologist. On October 24, 2013, Alyssa underwent a decompression surgery and was hospitalized for 4 days. She will need to follow up with the neurologist 6 weeks post op and then every 6 months from then on. Alyssa went back to Shriners in January 2014 to begin casting again and this xray showed a 94 degree curve out of the cast & 61 degree curve in the cast. Her next cast was applied on April 2014, showing a 96 degree curve. In July 2014, Alyssa went into Shriners to be fitted for her summer brace at which time an xray was taken. The X-ray at this time showed an improvement and she is down to 87* curved. We will go back to Shriners in September for another set of xrays and another cast will be applied. Due to the severity of Alyssa’s spine, growth rods and spinal fusion are not out of the question however we are delaying any surgeries and buying valuable growth time by using the casting method.
Antonio was born on December 6,1998. As soon as he was born, he didn’t look quite right so the doctors were rushed in and he was put in the NICU.
After days of testing he was finally clinically diagnosed wit Marfan’s syndrome. We were told that there would be heart, lens, joints, muscle and spinal complications to look out for in the near future.
Although, the diagnosis was wrong, he did end up getting scoliosis at 6 months of age. His over all diagnosis has not ever been found but we do know that it is some kind of connective tissue disorder. He has many symptoms of his condition but I will fill you in on the scoliosis journey. It has been the most difficult and longest, most painful part of his life and I include heart surgery as a far second.
Since Antonio has very loose joints and extremely low muscle tone and does not walk, his scoliosis progressed quickly and with a vengeance. At the time, 1999, we were told to brace him. Didn’t help. 6 months later his curve went from 30 degrees to 45 degrees. Then we were told that he would outgrow it….Three months later it was at 65 degrees.
__________________
Antonio is granted a wish by the Make A Wish Foundation to meet The Black Eyed Peas.
__________________
We changed doctors and he was put in a brace that he wore day and night with the hopes that the curve would hold and not get worse. He was braced until he was 7 years old when we decided that growth rods was our only choice. I fought to get him the VEPTR rods because they are a less invasive choice and his surgeon finally agreed However, he was put in halo traction first to get as much correction as we could before surgery. He stayed in halo traction for a whole year because we kept seeing improvement in the curve every time we went for an x-ray. He went to school with his halo traction and did everything while in traction. He was so comfortable because he didn’t have gravity holding him down and putting pressure on his spine. So then at eight years old the VEPTRs were implanted from his top rib to his pelvis.
Six months after the VEPTERs were implanted, his expansion surgery came next. Right after surgery we realized that his pelvis had been cracked by the pressure of the rods so one of the rods was removed. A few months later, his other rod migrated right through his rib and that one had to be removed as well. Antonio’s bones were much to soft to hold the rods and unfortunately we didn’t realize this until it was too late.
So, back to square one. He went back in a brace for several years and when he was 11 he went back in halo traction to prepare him for spinal fusion. At this point his curve was 106 degrees. He remained in halo traction for another year. I wanted to wait as long as possible so he could get as much growing time as he could. Again, Halo traction was his best friend and he was so incredibly comfortable. His curve went from 106 degrees to 45 degrees with traction.
At twelve years old he had his spinal fusion. It was a fourteen hour surgery . he spent the following 6 days on a ventilator and finally came off the vent and started the recovery process. Shortly after, he developed an infection and was put on a wound vac. A wound vac is where they fill the open wound with a special sponge and attach the sponge to a vacuum system that allows all the drainage to get sucked out of the wound and promote quicker healing. Every three days he was sent back to the O.R. where the sponge was taken out and replaced. It was a long horrible process that left him in the hospital all summer long.
Once we were done, we were sent home with a small wound that continued to drain for a whole year. He would not heal until the rods were removed from his spine but we needed time to allow his fusion to hold. After a year of keeping the wound issue at bay we went back to the O.R. to remove the rods. Again his infection returned and a new wound vac kept him the hospital for a whole other summer.
Once we finally closed up the wound and returned home he began to drain out of the same spot AGAIN!! We tried to heal it with help of antibiotics and wound care specialists but the following summer he was back in the O.R. to have another surgery to clean out the wound. Guess who came back? INFECTION…another wound vac and another summer in the hospital. Once that was finally over, the wound has been dry and closed and drama free.
We are still scared that the curve might come back because we had to remove the hardware that was keeping his spine in place However, I don’t see us going to the O.R anytime soon to put them back in.
Antonio’s scoliosis surgery has been a total nightmare. He was born too soon to benefit from the life saving Mehta Casting and it makes me so sad to think what if all these surgeries could have been avoided? At any rate, Antonio’s scoliosis journey is finally over (hopefully) but one thing about him is that he NEVER let any of this stuff get him down. He is an amazing boy with a great gift of positivity, patients and love.
Mehta, M.D. FRCS., MH. Growth as a Corrective Force in the Early Treatment of Progressive Infantile Scoliosis. J Bone Joint Surg Br. 2005; 87-B: p.1237-47 (more…)
Fletcher, Nicholas D., et al. Serial Casting as a Delay Tactic in the Treatment of Moderate-to-Severe Early-onset Scoliosis. Journal of Pediatrics. Volume 00, Number 00, 2012. (more…)
Cotrel, Yves and Georges Morel Revue de Chirurgie. The E.D.F Technique in the Correction of Scoliosis. Orthopedique et reparatrice de L’Appareil Moteur (Paris). Tome 50, 1964, no I, pp. 59 a 75. (more…)
M. Mehta, MD., FRCS The Rib Vertebral Angle in the Early Diagnosis Between Resolving and Progressive Infantile Scoliosis. J Bone Joint Surg Br. 1972 May;54(2):230-43. (more…)
Erin was born on February 2, 2002. It would have been her Maternal Great Grandmother’s 95th birthday, and Erin was the first girl on the paternal side of the family in 90 years!
At approximately 37-38 weeks, I had an ultrasound to make sure things were on track. There was a question raised from that ultrasound as to whether or not the baby had both of his/her kidneys. I was instructed to mention this to the L&D nurses after the birth of the child. We did not know until the birth whether it was a boy or a girl.
I was induced on Feb 1 at about 10:45 pm. This was due to my blood pressure going up and the baby was due on the 2nd anyway. L&D went fine, although the epidural was a waste of time – again. The same thing had happened with the birth of my son.
When Erin entered the world, and Dr. Lee announced “IT’S A GIRL!” John, my husband, said “Are you SURE?” Yeah, they were sure! After a few minutes of cuddling, the nurses took her to be weighed, measured and cleaned up. They all knew there was a question of a missing kidney, so while the nurse was cleaning her up, she said “She’s peeing!” What great news.
The next day, after an uneventful night, Erin was whisked away for an ultrasound. This confirmed, that in fact, she did only have one kidney. When they brought her back, I was filling out all the paperwork about lead, and hearing etc. The nurse said that even though we didn’t fall into the criteria for the newborn hearing test screening, we should probably have it done since kidneys, ears etc all form at the same time. We did and her hearing was fine.
At her 3 month checkup, her pediatrician noticed that her head would tilt to the right, he suspected torticollis, but wanted to wait till the 4 month check up because babies have such wobbly heads to begin with. At 4 months it was confirmed. Erin also had hip xrays because there was concern that her hips were not in alignment because one leg appeared longer than the other. Her hips were fine.
We started physical therapy for the torticollis, and when Erin was about a year old, her PT was rubbing her back and thought she felt a curvature of the spine. After xrays, we went to an Orthopedist who confirmed that Erin had congenital Scoliosis with hemivertabrae. After hearing the diagnosis, we switched orthos to Dr. Alvin Crawford (Dr. C), department head of the Ortho dept. at Cincinnati Children’s Hospital Medical Center (CCHMC). For about a year, we did the wait and see with xrays every 4-6 months. Erin was also seen by the Human Genetics dr, but it was discovered that none of this could be tied to Genetics. Dr. C also said Erin had Klippel Feil Syndrome, which is characterized by a low hairline and shortened cervical vertebrae.
When Erin was 2, Dr.C decided to put her in a Modified TLSO brace with Cervical Head Collar. this was not to help her spine, it was to stop the facial dysplacia that was occurring due to the torticollis. During this time, Dr. C explained what our options would most likely be: fusion, rods, or a new procedure that was still in clinical trials, the Vertical Expandable Prosthetic Titanium Rib or VEPTR. At this point we also discovered that Erin had fused ribs.
John and I were not thrilled with the idea of fusion and rods seemed so old fashioned. So I began trying to find out anything and everything that I could about the VEPTR. I found out that one of the trial sites was Boston’s Children’s Hospital. So I made a few phone calls and got Erin an appointment with Dr. John Emans. She and I flew to Boston with all her xrays and scans and met Dr. Emans in May of 2004. Based on what I had, Erin was not a candidate for the trials. But Dr. Emans did say he wanted to see her again if we ever visited (my family lives in Massachusetts).
When we returned, Dr. C was glad I had checked it out, but we were still looking for the best option for Erin. In 2004, Dr. C presented her case to three (3) different symposiums in different parts of the country to get other suggestions, advice, recommendations. In September 2004, the VEPTR was approved by the FDA!!!
In January of 2005, Erin had another 3-D CT scan. This one, Dr. C sent to Dr. Robert Campbell, co-creator of the VEPTR in San Antonio, TX. Dr. Campbell got back with Dr. C and said Erin would be a “picture perfect” candidate for the VEPTR, and would be perfect to be the first patient to receive it at CCHMC!!
On March 14, 2005, while I was on a cruise ship heading to Cozumel, Dr. C’s office called with the news that Dr. Campbell would be in town on March 22 to do Erin’s surgery!! John said yes – and did try to reach me on the ship to no avail. When I got back to my sister’s in Tampa, there was a message for me to call home. I was absolutely shocked when John told me the news. I flew home and spent the next week getting things set up for Erin’s surgery – having pre-op work done, getting coverage for me at work, finding someone to watch Patrick etc.
Everything worked out and Erin had her surgery and she came through it with flying colors!!! Protocol says the child will be on a ventilator for a day or two – Erin came out of surgery off the vent. . Protocol says the child will be in the hospital for 14 days or so, but we were only there 10. She was in PICU for 2 days then on the regular floor for 8 more. She was also a celebrity as the Cincinnati Enquirer did an article on her and we posted it on her door.
Her recovery has been great and it is amazing how tall and straight she stands. She will have to have expansion surgery every 4-6 months, but that should go just as well as the initial surgery. She is not able to play contact sports, but if you saw her on the playground with her friends, you would never know that she has had spinal surgery! Gail
In January 2011, our daughter Josefina of 6 months old was diagnosed with severe progressive infantile scoliosis. We live in Montevideo, Uruguay; a country of 3 million people, where cases like Josefina´s practically don’t exist, so effective treatments in our country weren’t t available. At first, doctor recommended us to travel to Argentina, were we didn’t get good results using braces, so the possibility of successive surgeries were in our close future.
At the age of only 12 months Josefina’s scoliosis, was already twisted to 90°, compromising her lungs and heart. At that point she got a virus in her lungs and we ended up in the intensive care unit for almost two weeks with respiratory problems. Searching for the best option for her, knowing that it was very important and necessary to obtain the best possible correction to prevent future thoracic insufficiency syndrome, we came across ISOP and as we read about Mehta Casting, we knew immediately that it was the option we were looking for our little girl. Without hesitating we got in contact with Heather who gave us information and the support we needed to fight for being able to reach Mehta Casting treatment for our daughter.
With the advice and support of Heather we began searching for options. We knew it was going to be a long road but were determined to fight to give our girl the best option.
On august 2011 we began our applications to get Josefina accepted as a patient in Shriners Hospital for Children in Salt Lake City. We contacted local representatives from Shriners here in Montevideo and began making the applications to get her accepted as a patient in Shriners Hospitals. We found amazing people that helped us during this process knowing that this was the best option for my daughter and that she deserves to have this chance in life. Luckily, in September 2011 we received the best phone call in our entire lives, telling us that finally Josefina had been accepted as a patient in Shriners Hospital!!! That phone call changed our lives forever; we can’t express how good it feels to finally know that Josefina was going to have this opportunity, to know that we had achieved our best goal ever: Fight for the health of our lil Josefina giving her the best option for her condition.
In November 2011 we finally started this great journey, and travelled to Salt Lake City to have our first appointment with Dr. Jacques D´Astous at Shriners Hospital. He agreed that Jose was a good candidate for Mehta Casting and that in her case was the best option that will contribute to postpone corrective surgery until she got older. November 26th 2011 was the date when Josefina´s first Mehta Cast was applied and they managed to get a correction in her twisted spine of 40 degrees (her curve was 92 degrees before cast and the xrays in cast showed a curve of 52 degrees!). We were so happy for this great result and also seeing Josefina recovered so well, seeing her running around in her new cast!
Since November 2011, we´ve been travelling every 3 months to Shriners Hospital in Salt Lake City. Josefina is now 4 years old, she is wearing her 12th cast and is a healthy and happy girl. This alternative method to surgery, Mehta Cast, is allowing Josefina to grow older, with a good quality of life, buying valuable time and delaying surgery the more we can.
We would especially like to THANK ISOP and Heather for giving us the information and support we needed. If it hasn´t been for her advocacy and work we would have probably never know about Mehta Cast. We also want to thank Salt Lake City Shriners Hospital´s staff. From the very first moment we felt really comfortable on how Dr D´Astous and his team treated our daughter, their professionalism and excellent reputation made us feel absolutely convinced that we were on the right track. Every single person that is in touch with our daughter while we are in the hospital is just WONDEFRUL. Starting with Dr D`Astous, excellent person and professional, always explaining to us how Josefina is doing and taking the time to answer questions about her future. His team is also great, and compromised with every little one, caring and explaining every step they do. We would also like to mention the excellent work Anaesthesiologists do, their professionalism keep us calm knowing she is in really good hands. Also nurses, psychologist, and all the staff in Shriners Salt Lake City are just amazing and caring with our lil Josefina, making each procedure the less traumatic for her. We felt really blessed to have this opportunity for her, knowing that we still have a long journey to go, but feeling confident that we are on the right path.
This is our family priority, to fight for Josefina´s health, giving her a good quality of life while going through this process. We are receiving the help of our family, aunts, uncles, grandparents, friends and our community. They are helping us afford the cost of travelling every 3 months and we are really thankful for that too
We still have a long way to go and Shriners Hospital is our main allied on this journey. This gives us strength and hope in Josefina`s future, knowing that she is receiving the best treatment ever, and that we couldn`t have given it to her if it wasn´t for the help of Shriners.
In June of 2012, I noticed Starla’s back was forming oddly. I didn’t know at the time that was a rib hump. She was nearly 6 months old then. Many blew it off and I didn’t know if it was a big deal or not. In December, 2012 my chiropractor ordered an x-ray of her back. I took the x-ray to her pediatrician who diagnosed her with infantile Scoliosis. She was days away from turning one year old. We were blessed by the fact that her pediatrician was honest enough to tell me that he didn’t know who to send her to. As soon as I got home, I googled Infantile Scoliosis and found ISOP. The following week I was in contact with a hospital which applies the Mehta Cast to patients and had our first appointment January 2, 2013.
It was very hard to go through these first few appointments. We were told Starla’s curve was 30 degrees with rotation and the doctor wanted to wait and see how her scoliosis would develop as she grows. We understood the wait and see and were hopeful that we would see improvement. But we also questioned at what point we decide to cast. She continued to grow but the curve continued to stay at 30 degrees. Being a Christian married couple, we always make big decisions together. This decision was a challenge for us. One of us had faith God would heal her without treatment. The other felt God telling us to cast her. It was a challenge to get on the same page it required several difficult conversations. Ultimately, we decided that if the doctor recommended casting, we would move forward with the treatment.
Starla’s first Mehta cast was applied May 21, 2013 at the age of 16 months with her pre-cast x-ray revealing a 37 degree curve. It was a rough day as I assume it is for every family. We were filled with emotions. Emotions of thankfulness that she was getting the treatment that could cure her, emotions of grief that she needed to be in such a hospital getting treatment. Fear of how our lives would change and hopeful that we started treatment early enough.
The procedure went much faster than I had anticipated. The doctor was paging us after just 15 minutes. I panicked because I thought something had to have gone wrong for them to page us so quickly. When he entered the room, he told us everything went very well. He got her curve completely straight and rotation completely straight, too! What a miracle! We had been warned prior to casting that he would focus on the rotation with the first cast and not to expect great improvements with the curve. So, to have both completely straight was astonishing! It confirmed in our hearts that we did the right thing in treating her early.
We are currently finishing up our first full week in our first cast. Starla is the same person she was before. She plays and laughs. She eats and sleeps. She falls over more and can’t get up. She has learned she can’t pick toys up off the floor and whines until she gets our attention to hand her a toy. She has learned to roll over in her crib but is still not strong enough to push herself up. I feel that we are reliving the milestones we accomplished nearly a year ago. But that is ok. She will figure these things out and we continue to find little ways to help make life a little more comfortable. We have given her a sponge bath and have learned how to floss. I feel we have learned about all we need to in this first week. It was scary at first but I am trusting that it will get easier and easier and become more normal.
I haven’t thought much about the next cast. I know to expect her curve to return most likely to the 30’s again out of cast. I am hopeful she will become straight again once in the second cast. At that point, she will be 18 months old. I plan to start charting her numbers in and out of cast. I am hopeful we will see the trend to start dropping and continue that downward slide to zero. I am personally hopeful she will be straight out of cast in a short one to two years. I know there are no guarantees but that is where our faith continues. We have faith that God brought this treatment to us so quickly and that He will use it to heal our daughter completely. We have faith that she will be a walking testimony of God’s healing power.
To any parents out there just beginning to get your child evaluated, please keep strong. Have hope and push for treatment. If you are a parenting team, hold on tight to each other and don’t let the stresses of the condition divide you. Your little child needs you both. If you find a doctor dragging his feet in treating your child, PLEASE get a second or third opinion from another Mehta Casting specialist. Reach out for help if you are not sure what to do. There are many families out here who have left their own foot prints in this scoliosis world and would love to take your hand and give you a tour of the possibilities. Your child can be cured. It isn’t a guarantee BUT the sooner your child gets treated with a Mehta Cast, the better outcome he or she will have. So, let the tears flow when you need to, but forge ahead in treatment. You can find a great support system if you reach out and ask.
Devyn was born October 3rd, 2005. The pregnancy and delivery were anything but normal. I had a sub-chorionic bleed until my 5th month of pregnancy that almost caused me to miscarry. The delivery started out normal until I started to push…. He got stuck twice and then was not breathing when he was born. After they resuscitated him he was fine except for his purple and blue bruised face.
Devyn seemed very healthy as a baby except for a milk allergy. He rolled over early, sat up at 5 to 6 months, and started crawling at 9 months, and walking at a year. It was then when we noticed something alarming. He stood in front of me one day in just his diaper, when I noticed that his back looked different. I mentioned it to my husband who knew it was there, but found it easier to pretend there was nothing wrong. We had a family get together for Thanksgiving, and I asked my mom and sister what they thought. They too said it was not normal and something was wrong.
The first week in December we had an appointment with his pediatrician for his shots, and I asked her to look at his back. She said that it was curved and that we needed x-rays and to see an orthopedist. Sure enough, the x-rays showed that he had scoliosis with a 24-degree curve in the lumbar area. The Orthopedist wanted an MRI to see if the spine was tethered at the base. So on January 11th we had the MRI done, what an experience—that drained us all. The results showed that the chord was not tethered and he had abnormally shaped cerebellar tonsils. The Orthopedist said that the pediatrician needed to refer us to a neurosurgeon and that she didn’t want to do anything at the time for the scoliosis, and to come back and see her in 4 months. So we saw our pediatrician again and she said we were not going to watch and wait. She sent us to Children’s Hospital in Denver to see an orthopedic surgeon for the scoliosis and a neurosurgeon.
We saw the orthopedic surgeons PA on February 2nd, 2007. He told us that he could definitely do something to help correct the scoliosis from progressing. He explained the early treatment process with the POP jackets and how it works. He said that we had to see the neurosurgeon first to make sure there were no neurological problems that would be affected by the casts.
March 7th we saw the neurosurgeon, who informed us that Devyn had Chiari Malformation along with his progressive infantile scoliosis. Chiari Malformation is where the lower part of the back of the skull does not form properly and is flat rather than curved. This pushes on the cerebellum (part of the brain) and causes the cerebellar tonsils at the base of the brain to descend downward into the spinal canal instead of under the skull and can cause pressure. This can cause the balance to be very unsteady, headaches, numbness, and in severe cases paralysis. He did not believe that the two were related because the Chiari malformation was not severe and not causing pressure on the spine. He told us at first that he wasn’t sure that surgery for the Chiari was necessary. He then asked if he could keep the MRI and share it with his colleagues to get their opinion. Of course, we had no problems with that—I want the best for my baby. The week after our appointment I received a call from the doctor himself. He explained that he shared the films with the other doctors and they decided that the surgery was necessary to make sure the two were not related.
On March 29th, 2007 Devyn had decompression surgery for the Chiari Malformation. They opened up the back of his neck and cut out half of the C1 vertebrate, and took out the left cellebellar tonsil, and cut the right one back. They also opened the Dura, which is on the back of the brain. He spent four days in the hospital, and is doing great. We have noticed small improvements of things we never knew were wrong with him. His balance has improved greatly; he used to scream in the car non-stop and now is not bothered by car rides. These are things we didn’t know because he was too young to tell us.
Although these things are better his scoliosis had not improved. They did x-rays on March 7th after his appointment with the neurosurgeon. His curve had progressed to 37-degrees and his rotation was at 30 degrees. His right foot turned in like a pigeon when he walked and seemed worse every day. His curve also looked like it was getting worse.
We were finally cleared for Devyn to get his first POP jacket on May 9th 2007. They did not do x-rays when they casted. The doctor tries to expose them to as little radiation, as possible. They were figuring the curve at a little over 40 degrees at the time he got his cast. He did better than we had expected in the hospital, a little mad at first but got used to the idea that it wasn’t coming off. The first week was a little rough as he had a hard time adjusting and moving in the cast. He couldn’t bend over or sit on the floor and sleeping was really hard at first for him, as well. After the first week he improved, and he learned how to accomplish something new every day. After two weeks he was back to his old self, getting into everything and climbing on everything.
On June 8th we went in for his first x-ray in cast. The doctor walked in and said, “refresh my memory, what did we start at?” He handed us the x-ray and told us to guess….. I was amazed, the x-ray looked almost straight! He said it measured 15 degrees and hopefully one more cast and a good growth spurt should do the trick. On July 6th Devyn received his second cast. They didnt x-ray on the day of casting this time either, they used the numbers from his last x-ray. On August 9th they took his in cast x-ray. This time it measured 10 degrees. As you can imagine we were very happy. The doctor said lets do one more cast to see if we can go any lower or if we hold this degree.
On September 10th Devyn received his third cast. We followed up on October 5th for his x-ray. The curve was holding at 10 degrees. We are still so happy because it’s better then when we started! On October 27th they took off Devyn’s cast and molded him for a brace. He received his first brace on October 31st. They did an x-ray to make sure the brace was adjusted correctly. He still measured 10 degrees. He wears his brace all the time except for bath’s and swimming. We went in on November 30th for his first x-ray with the brace, this time they had us take an out of brace x-ray. He is still holding at 10 degrees.
The D-shaped window on the back of a Mehta cast actively assists in the derotation of the child’s most prevalent curve with every breath the child takes. The D -shaped window should always be placed on the concavity side of curve, not past the midline. This special window allows the oblique ribs on the cavity side to grow out of the window, while the ribs on the convexity side are molded down to improve overall body shape and decrease rib hump.
The most effective way to determine the nature of your child’s curve is to have a pediatric orthopedic surgeon measure the Rib Verteral Angle Degree (RVAD). This simple, free and effective measuring technique uses a pencil and a ruler and was developed by Dr. Min Mehta in the early 70s.
If the RVAD is more than 20 degrees, the child’s scoliosis is considered to be PIS and progressive in nature. Immediate treatment with Mehta’s Growth Guidance Casting (MGGC) is indicated.
If the RVAD is under 20, it’s considered self-resolving and must be monitored closely with a follow up x-ray within 2 months.
Lily was born April 12 2004. She was diagnosed with plageocephaly at approximately 8 months of age. She was placed in a corrective helmet by the orthopedic physician, which was worn 24/7 for 4 months. This corrected the flatness of her head and restored its shape.
At 13 months of age, Lily had just started to walk. We noticed that she only had fat rolls on one side and that one shoulder drooped just slightly lower than the other. Up to this point, no mention had been made to us about scoliosis by her pediatrician or her orthopedic physician. We suspected, however, that scoliosis may be the problem. We took her to her pediatrician and told her what we suspected and asked that her back be radiographed. The radiograph confirmed our suspicions. She was referred back to the orthopedic physician who ordered an MRI to rule out congenital problems, as well as more radiographs. In one radiograph, Lily being her sometimes less than cooperative self, shifted just right and brought one of her hips into the field. A very astute x-ray tech noticed that the hip was dysplastic. More radiographs confirmed the diagnosis of bilateral hip dysplasia. This we were told was an unusual situation. The orthopedic physician informed us that traditionally one of these problems is usually treated at the expense of the other. He said he wanted to treat them together which to his knowledge had never been done. He recommended a Spica brace and a TLSO brace to be worn together, although he admitted he was not certain how that would be done.
At this point, I spent every waking moment researching treatment options and outcomes. This eventually led me to www.abilityconnectioncolorado.org/newsite/infantilescoliosis. They sent us a video and other information. After careful scrutiny, and much deliberation, we felt like early treatment would be the best option for Lily.
Lily was admitted to Shriner’s Hospital in Salt Lake City. Her dr. in SLC also wanted to treat the hip dysplasia and the scoliosis together. She was first casted September 13th 2005. She was placed into a modified plaster SPICA/Risser cast to treat both the scoliosis and the dysplasia concomitantly. This was the first cast of its kind. She wore this cast for 2 months. All subsequent casts have been of plaster, and done on a size appropriate casting frame. Eventually, Lily was placed in a Craig Hip abduction orthosis to be worn during naps and at night.
Her progress is as follows:
September 13th 2005:
Pre-cast: COBB = 46
RVAD = 30
In-cast: COBB = 8
November 16th 2005:
In-cast: COBB = 14
March 6th 2006:
Out-of-cast: COBB = 20
In-cast: COBB = 11
June 28th 2006:
Out-of-cast: COBB = 20
In-cast: COBB = 5
Oct 5th 2006:
Out-of-cast: COBB = 7
In-cast: COBB = 0
Lily will undergo one more casting in December 2006 to be worn until April 2007. She will then be placed in a TLSO brace for the remainder of her treatment. Her hips have not made much progress until the Oct visit when slight improvements were noted. There has also been no regression or dislocation. Her hips will be monitored until the age of 4 or 5 at which time she will undergo surgery for the dysplasia if the hips have not ossified and formed correctly.
We are very grateful to have found the ISOP (Infantile Scoliosis Outreach Program) for the hard work that’s been done in keeping us all connected and informed. We are also very grateful to our Dr. and the wonderful staff at SLC Shriner’s Hospital for all their hard work and dedication.
Siobhan was born June 9th 1999 in Vancouver, Canada, 4 days late. Her birth was normal. We noticed at about 4-6 months old that she didn’t bear weight and, when her feet were on a flat surface, they pronated (rolled inwards) quite severely.
Our family doctor sent her to see an orthopedist at our Children’s Hospital, who explained that she would need orthotics when she started walking. Then, upon closer examination, he remarked how long her fingers and toes were. He referred us to a genetic doctor to have Siobhan checked for the Marfan syndrome.
The genetic doctor sent us to an Ophthalmologist for a ‘slit lamp’ eye exam and to a Cardiologist for an echocardiogram and x-rays of the hands, feet and spine. During this spine x-ray, Siobhan’s scoliosis was detected. She was 20 months old, and her COBB measured 23 degrees lumbar and 17 thoracic. Our orthopedist at the time felt it would get worse as she grew, but recommended the “wait and see” approach. Siobhan had an x-ray every 3 months for 9 months with no change. It was then recommended that we cut down on the x-ray exposure, and she would be seen every 6 months.
About two months after that decision, I noticed in a recent photograph that one of Siobhan’s shoulders was markedly “dropped” (uneven). We decided not to wait for another 4 months, and took her back for another x-ray. Her lumbar curve had increased to 35 degrees and her thoracic to 26 degrees. That’s when she went into her Boston TLSO, which she wore 23/7 for 9 months, with her curves maintaining at approximately 35°/26°.
But by one year later, her lumbar curve was 45°, and I was growing very concerned. Our orthopedist had originally told us that a spinal fusion would probably be necessary when she reached 12 years old, but later mentioned that it could be necessary when Siobhan was 10 years old. By our last visit, when Siobhan had faithfully worn the brace for 23 hours a day, 7 days a week, he was suggesting fusing her spine at 8 years old.
This is when we looked into serial casting as an option. Thanks to the Infantile Scoliosis Outreach Program’s website and the information I learned through Heather Hyatt, we found the only doctor, Jacques D’Astous, MD, who was willing to cast her in a plaster of paris cast (POP jacket). He applied Siobhan’s first plaster cast in June, 2004, at Intermountain Shriners Hospital in Salt Lake City, Utah, when she was 4 years old. At that time, her curves were measured at 32° lumbar/20° thoracic (in the cast). Her second cast was applied at the end of August 2004, reducing her lumbar curve to 8°/thoracic 17°. Her third cast saw her lumbar curve at zero/thoracic 25°, (measured on x-rays while in the cast.)
She is currently back in a Boston TLSO, which she wears 16-20 hours a day, and is getting lots of physiotherapy and swimming. Dr D’Astous will continue to follow Siobhan every 3-4 months and, when he feels her curves are increasing, will apply another series of POP jackets to buy as much time as possible for her grow.
Siobhan’s diagnosis is a “connective tissue disorder/possible emerging marfans/possible MASS phenotype.” We all know this means that her spine may just keep on curving, but we will all do everything we can to stall any surgery until she is older, much older.
Thank you for reading my little girl’s story. And if you have any questions please feel free to email me at jabostock@yahoo.ca
January 2008 Update
Siobhan continued to wear a brace 16 hours a day, until November 2005, when her doctor suggested she be evaluated for VEPTR (Vertical Expandable Prosthetic Titanium Rib).
We’d done a lot of research and believed that this fairly new procedure would help Siobhan, and improve the quality of her life even more.
The Mehta casting had bought us time, reduced Siobhan’s curves, and had helped correct her rotation, but her connective tissue disorder meant that we needed something more. Her doctor explained that these VEPTR’s would literally act as an “internal brace”.
We knew this surgery would be invasive in the short term, and a major commitment in the long term. But we trusted Siobhan’s Orthopedist.
In May 2006, Siobhan was the first child to receive the VEPTR dual hybrid (attached to her iliac crests) at the Shriners, Salt Lake City. Her curves went from 34 degrees thoracic/ 49 degrees lumbar to 0* thoracic/ 12* lumbar – All the doctors were very excited! Us too!
Siobhan received a confirmed diagnosis of “Emerging Marfan Syndrome”, by the Genetics Dept of our Children’s Hospital in January 2006.
Her first expansion of her dual VEPTR’s in November 2006 went smoothly – 6 months after the initial implants. But by January of 2007 we started to notice that Siobhan seemed unable to stand straight anymore – She’d acquired a “stoop” that she didn’t have before.
We emailed back and forth to her doctors in Salt Lake City, who informed us that we may need to look at moving these 2 VEPTR’s from the pelvis, as for some children, this stooping was becoming a problem. Both doctors agreed that relocating them to the laminae should help Siobhan.
Back.com definition: Laminae
The laminae are two flattened plates of bone extending medially from the pedicles to form the posterior wall of the vertebral foramen
Intermountain Shriners found Siobhan an appointment at the end of April 2007, where her surgeon moved the pelvic devices. Surgery was harder than expected, but as always within a couple of weeks, Siobhan bounced back!
Siobhan is doing well in Grade 3, tap dancing and playing the piano – Having the wonderful childhood she deserves.
Kylie Anne Lether was born August 8, 1997 in Salt Lake City, Utah. She weighed 6lbs. 10oz. and was 21 ½ inches long. She was born with Infantile Idiopathic Scoliosis and Developmental Hip Dysplasia. Her back had a big hump on the left side, which was her spine lifting her shoulder blade up. Her hip sockets were straight instead of curved and there were no femoral heads. Doctors are sure both of these problems were caused by the way she was positioned and had ran out of room in utero. Kylie was full term, breech and on a diagonal facing outwards. I was told that she had to have been in that position for quite some time to have caused such damage.
Because she had both problems that couldn’t be focused on at the same time, her orthopedic doctor focused on the most severe, which were the hips. We were told that if the hips were not corrected as early as possible, she would have to undergo many surgeries involving cutting of the hip sockets, metal plates and screws. There would also be the possibility that she wouldn’t walk normal or even at all. In the mean time, her scoliosis was progressing. It was already in the high 20’s.
At two weeks old, she was placed in a Pavlik harness brace and then when she was four months old, she had her first of many Spica casts applied. After five weeks in her first Spica cast, she was hospitalized for two weeks with bacterial meningitis from an ear infection that didn’t respond to antibiotics. She was also misdiagnosed many times. When she was finally diagnosed, we were told that they didn’t think she was going to make it. If she did make it through, she would be mentally retarded, blind, deaf, and not live a long life. To treat her meningitis, doctors had to cut the Spica cast off. While being treated for the meningitis, her right leg had become dislocated and she needed surgery to get it back into the socket. During this time, we learned that she had a Duplex Kidney, which is a kidney that measures a half length longer than the other. She underwent testing to determine if the kidney was functioning normal, which it was. We also learned that she was deaf in her right ear. We all assumed that it was caused from the meningitis; we later learned through a MRI that her ear bones in the right ear had abnormalities from birth.
Kylie is a fighter!! She pulled through the meningitis with some possible nerve damage that makes her muscles weak and almost impossible to build strength. The left side of her body is affected more than her right side. She ended up being in Spica casts for about five months. Her hip sockets developed normally and the femoral heads developed, as well.
Finally, her doctor was able to focus on her spine. By this time, her curve was 45 degrees. She was immediately placed in a TLSO brace. The brace corrected the curve to 34 degrees. We would go to regular follow up appointments and the curve always stayed 34 degrees. When she was 3 years old, her curve started progressing. It was progressing very quickly. Her curve was now 52 degrees. Her doctor discussed Risser casting with us and we agreed to try it. She wore two different casts for three months and her curve was back down to 34 degrees. After the Risser casts, she went back into a TLSO brace. At that time, we started discussing with her doctor some of the other non-surgical options because we knew it was just a matter of time before her curve would progress. He told us about the Halo Traction procedure. The Halo Traction is the gentle pulling of the soft tissue (joints and muscles) to help straighten the spine. Weights are hung from a rope woven through a pulley system to a carabineer attached to the top of the Halo. The traction gently pulls against the child’s body weight to straighten the spine, gently and nonsurgiclly. The Halo Traction Treatment for progressive infantile scoliosis was a new procedure to the U.S. and at the time was only available at Shriner’s Intermountain Hospital in Salt Lake City, Utah. Fortunately, that was the Shriner’s Kylie went to and we only lived 20 minutes away.
We read a booklet published by Shriner’s Intermountain about the Halo Traction procedure that showed pictures and told us how the whole thing worked. We also watched the video with Olivia and Breann, two of the first children in SLC to benefit from this non surgical procedure. After reading and watching, I FREAKED!! I knew that one day she would have to have this procedure done, but I didn’t think I could put her through that after all she had already been through. My husband and I decided that we would allow her doctor to do the procedure when it became necessary. We knew it was the only way to avoid early fusing of the spine and we figured that we would have enough time to get use to the whole idea, before she had to have the Halo. Five months later her curve was at 70 degrees, HALO TIME! I was so upset and couldn’t stop crying. Kylie walked up to me and asked why I was crying and then said, “Oh, it’s because my back got worse huh? Well that’s ok mom, because the front of me is not broke.” And then went back to playing with some toys. That’s when I realized that I needed to pull it together. My child was stronger than me!
Kylie started the Halo Traction in May 2002. She had to stay at Shriner’s with her Halo for 2 months. She was unbelievable! She never complained or wanted her halo off. She loved it and couldn’t wait to show it to everyone and tell them that she was an angel. She never wanted her doctor to take it off.
She had a wheelchair and a walker that she used with the Halo. When it was almost time for the Halo to be removed, we needed to decide on what was next for treatment. I was terrified to have the Halo removed because I knew that with the Halo on, her spine couldn’t get worse. The Halo traction corrected her curve from 70 degrees to 24 degrees. The last time her curve was close to that, was when she was about four months old. We knew that if we had her placed into a TLSO brace again, her curve would progress very quickly and we didn’t want to loose the great correction we gained from the Halo Traction. In talking with her doctor, we learned about Subcutaneous Growth Rods. We were very nervous to try the Growth Rods because we didn’t know what the outcome would be and knew the risk of spontaneous fusion to the spine at the attachment points. They would have to surgically lengthen them about every six months as she grew. We were also told that we could have the rods removed at any time if we decided to, and could go with some other treatment. We decided we would give them a try.
Kylie had her Halo removed and underwent Subcutaneous Growth Rod surgery. I was amazed at how quickly she recovered from the surgery and that she didn’t have much pain at all. She immediately took to her new rods, although she was sad to have her Halo taken away. She called them her special rods. When she had her Growth Rods lengthened for the first time, six months later, her curve was still 24 degrees. Every time the rods were lengthened, a couple of degrees would be lost. After two years with the Growth Rods, she started developing Kyphosis above the rods. The Kyphosis progressed very quickly, to 95 degrees. In May 2004, the Growth Rods were removed and she underwent the Halo Traction for the second time. Kylie was so happy to have her Halo back, and I have to admit that I was too. She did so well with the first one and the correction we got was great, how could I not be happy!
Kylie was in the second Halo for two months. Because she is older, her spine has become rigid, and Kyphosis is harder to correct. So, we didn’t get as much correction as last time. Her scoliosis was 45 degrees corrected to 40 degrees and the Kyphosis was 95 degrees corrected to 56 degrees. After the second Halo was removed, we decided to have her placed into a plaster Risser cast, this time with neck support to help with the Kyphosis.
She had her first Risser cast with neck support on for about ten weeks. We didn’t gain any correction in it. She had the second cast applied. We did gain some correction this time. The Kyphosis has been corrected to 45 degrees, 11 degrees of correction. She had that cast on until November 2004. When the cast was cut off, her spine instantly regressed back to 49 degrees. That same day, while we were waiting for her brace with neck support to be completely finished, her spine progressed from 49 to 60 degrees in just six hours.
In March 2005, she had her first orthopedic appointment for x-rays since she’d been wearing the new brace. She measured at 60 degrees, still. After her orthopedic appointment, we met with the neurologist at Shriner’s to have Kylie evaluated. She read her history and asked a lot of questions, then examined her. She then told me that she didn’t think Kylie’s physical disabilities and muscle weakness were caused by the meningitis she had at five months of age. She believes Kylie has a type of nonprogressive muscle myopathy, which she was born with. I didn’t know what to say, that wasn’t at all what I expected to hear. I couldn’t help thinking, why wasn’t this noticed earlier, like when she was born. From the time she was two weeks old, she had been in a brace or cast for her hips and then in a brace or plaster cast for her scoliosis. She was not able to physically develop when she was suppose to and then having meningitis at a very young age, no one ever noticed that something else was wrong with her. It was assumed, that the meningitis was the cause of her physical disabilities and lack of muscle tone.
The neurologist scheduled Kylie for a MRI of the brain, to see how much and how the meningitis had affected her brain. We received the MRI results that same day. The scans showed that her frontal lobe was affected the most. The frontal lobe was covered with many large white patches, which are basically dead parts of the grey matter due to lack of oxygen. Her entire brain is covered with smaller white spots. The doctor at Primary Children’s Hospital pulled up her past CAT scans to look at them. The first scan was when she was admitted with meningitis, had no white spots anywhere on the brain. The second set of scans were taken three days later, had all the white spotting. Fortunately, the damage wasn’t bad enough to have taken any functions away, just enough to alter some things a little. Kylie is a very smart kid. Sometimes she needs constant reminding to do certain things. She has a hard time concentrating at times. These are a few things she will have to deal with. Kylie will also undergo a muscle biopsy the next time she is sedated for a plaster cast or Halo traction, to determine what is exactly wrong with her muscles.
In May 2005, Kylie was one out of fifteen children selected to be a part of the first ever, Early Treatment Trial Project (ETTP) training conference, for progressive infantile scoliosis. The conference was held at Shriner’s Intermountain Hospital in Salt Lake City, Utah. It was sponsored by the Infantile Scoliosis Outreach Program, a service of Ability Connection Colorado. The conference was held to train doctors in the early treatment casting technique from the pioneer of this treatment, orthopedic physician, Miss Min H. Mehta, MD, FRCS. Miss Mehta retired from the Royal National Orthopedic Hospital in London and Stanmore, England.
Miss Mehta examined each child with the doctors and practitioners observing her examination techniques. We learned a lot of new things about Kylie, some good things and some not so good. We learned that the only benefit Kylie will ever have from casting is to hold her curve where it is, no permanent correction. Also the casts can not untwist her severely twisted spine. Kylie’s spine is too rigid. That was very upsetting to hear. Miss Mehta was
however, able to give us great relief in knowing that our decision of growth rods did not cause Kylie to develop kyphosis. She told us that her vertebrae in
that area were already twisted and that she would have developed kyphosis anyway. Miss Mehta told us that because her spine is so rigid and it’s been like this for so long, it might start to self fuse. She highly recommended that Kylie needed to spend up to 4 hours a day out of her brace doing special exercises and stretching techniques which she showed us, in hope that it will loosen her spine and avoid self fusing. I was terrified to have her out of her brace that
long, she progresses very quickly. When her last cast was cut off and we were waiting for her brace to be finished, her spine went from 49 degrees to 60 degrees in just 6 hours. Kylie’s been out of her brace every day for 2 to 4 hours doing constant stretching and exercising.
Kylie had her orthopedic follow up at the beginning of June 2005. We were quite nervous for this appointment because the outcome of this appointment would determine if she would undergo her third Halo traction. Kylie doesn’t have to undergo a third Halo for now. At her appointment three months later, her spine measured at 60 degrees in the brace. In June 2005, her spine measured at 55 degrees out of brace! We were shocked!
I believe that the special exercises, stretching techniques, and spending that much time out of the brace to do them, is the reason she is at 55 degrees now. She has also been doing a lot of swimming in our pool. Kylie is now able to get herself off the ground with no help from anyone or anything. We were told she may never accomplish that, she did!
Kylie will continue to wear her brace with neck support and enjoy the summer in her swimming pool. Kylie has been wearing this brace since November 2004. It was believed that this brace would not hold her spine at all. This brace has helped her spine from progressing! Kylie has her next orthopedic appointment in October 2005.
2005-2007 Update:
Kylie had her orthopedic appointment in October 2005, her scoliosis measured 60 degrees. She also has a lot more rotation. On February 6, 2006, she underwent her third Halo Traction. She was very happy! She was also able to have a muscle biopsy. The muscle biopsy came back positive for myopathy, no specific type. Her myopathy is non-progressive, although if she doesn’t stay active and work her muscles, they will atrophy. She will be unable to regain the muscles. The muscle tone and strength she has now, is all she’ll ever have. It is uncertain at this time how this will affect her as she gets older and bigger.
Two weeks before her Halo was to be removed, she was approved to undergo a procedure called the VEPTR. (Vertical, Expandable, Prosthetic, Titanium Rib.) VEPTR is a surgical procedure that consists of two rods that are made of titanium. They are adjustable, and are placed on the outside of the rib cage. They are attached to a set of top ribs and to the pelvis, she has one on both sides. The VEPTR is internal bracing for the spine and must be surgically adjusted as she grows, approximately every six months.
This procedure couldn’t have come at a better time. We had been told that plaster casts were no longer an option, the Halo Traction was not correcting much at all, and back braces alone would never hold her spine. Eventually, her heart and lungs would suffer. At this time, a spinal fusion was not an option either. Kylie was nine years old, she is small for her age. Her Duplex kidney causes her internal organs on her left side to be crowded. The bottom part of her lung it folded under and her heart has been shifted out of its proper spot. If the growth of her torso is stopped, the internal organs will become even more crowded and this would be life threatening.
Kylie had her VEPTR dual hybrid surgery on April 3, 2006 at Primary Children’s Hospital in SLC. She was transferred there from Shriner’s Intermountain Hospital, in her Halo Traction. The co-inventor of the dual VEPTR hybrid performed her surgery with assistance from her orthopedic doctor, since birth. She did wonderful, everything went as planned. The VEPTR has done amazing correction for her. With her spine being so rigid, we were all surprised how much the VEPTR dual hybrid had corrected her spine. After two months in the Halo Traction and before the VEPTR, her scoliosis was at 63 degrees. After the VEPTR it was at 42 degrees. Her kyphosis was 70 degrees before the VEPTR, after it was ZERO! Her back was so flat, it wasn’t even that flat when she was born.
Four days after her surgery, she was transferred back to Shriner’s Hospital, where she had been staying for two months prior to surgery, to finish recovering. She was able to go home the following week. Every six months, she will return to have her VEPTR expanded by the brilliant surgeon surgeons in SLC..
In August 2006, four months after her VEPTR was implanted, the left side came off the rib. She went in for surgery later that week to have it re-implanted. Her doctor felt like that the reason for it coming off was that there was too much tension on the VEPTR in that area where the kyphosis was being held to zero degrees. During surgery, he released some of the kyphosis and moved the VEPTR down to the next rib. A week later the VEPTR on the right side came off and broke the rib. Her doctor re-implanted the rod that had eroded through the rib and reattached it on the rib below, like the other side had been. He also went ahead and expanded the VEPTR, she was only a month away from her expansion date.
On October 30, 2006, Kylie underwent soft tissue releasing of the hips, back of both knees, and her left shoulder. With myopathy of the muscles, her soft tissues don’t grow at the same rate as her bones. The soft tissues become contracted like tight rubber bands and require to be released with surgery. This is something she will have to do again until she is done growing.
Kylie hit another obstacle with her VEPTR. Her kyphosis had drastically progressed right above where the VEPTR is implanted to the ribs. Her upper back and neck had completely collapsed. This was a complication due to her myopathy. She doesn’t have the muscle strength to hold up any unsupported parts of her spine, therefore that part of her spine collapses. Both of her doctors agreed that she needed to wear a brace with neck support so her neck didn’t worsen and get her on the schedule at Shriner’s for another Halo Traction as soon as possible.
On January 8, 2007, she underwent Halo Traction number four. She was able to keep the VEPTR in while being in traction because the area that needed to be straightened was above the VEPTR. This was the first time a Halo Traction was done with the VEPTR still implanted. Everything went very well. Her upper back and neck were corrected back to the way it was before collapsing.
Now the plan was to expand her VEPTR and move it to higher ribs to get better control, put her in a Halo Brace for two months while she healed from the surgery, then put her in a brace with neck support.
On February 8, 2007, she had her VEPTR expansion and revision surgery. Things did not go as planned. Kylies surgeon was unable to move the VEPTR up any higher. Her kyphosis would not allow it. He couldn’t get the left side to the next rib and the right side he couldn’t get it to stay on the rib. It immediately popped off and broke the rib. The VEPTR was put back on the original ribs as before. Kylie stayed in traction with only half of the weights as before, until the end of February. Then the Halo Brace was put on and she went home.
Kylie was in the Halo Brace for three weeks, we noticed that her VEPTR on the left side was starting to bulge out more than normal. I took her to get an x-ray to see if the VEPTR was coming off or if it was already off. The VEPTR was still on, but barely. This was happening because her upper back and neck, once again, was collapsing. No one could believe that it had collapsed with a Halo Brace on.
On March 26, 2007, Kylie underwent her fifth Halo Traction to correct her collapsed spine once again. She was very happy to have her Halo Traction back. Kylie told us that the reason she loves being in the Halo Traction, was because it allows her to move and do things she can’t do without it, because of her weak muscles. She is very proud that she holds the record for having the most Halo Tractions for spine straightening in the United States, by a long shot.
On April 23, 2007, we had no other options but to have the upper part of her spine that continued to collapse, fused. She underwent a fusion from T1 to T5. Her surgeon since birth performed the surgery. The area was reinforced with wire and she has a rod that runs alongside it. Her skin was closed with forty staples. Her skin has been cut so many times in that area that it is solid scar tissue. The staples hold the skin together better. The Halo Traction was left on for two more weeks with half the weights.
Kylie’s recovery was amazing! She was up and on the go four days after the surgery. She finally was able to go home on, May 11, 2007.
Since being home and recovered, she is a lot weaker than she was before. Although she was very active in her Halo, being in traction for so long had allowed muscles that couldn’t be used, weaken. She can no longer do some of the things she used to do before the last two Halo Tractions. This is very devastating to us. She continues to do therapy on a daily basis, to maintain what muscle strength she has left.
On September 17, 2007, she had her VEPTR expansion and another revision of the left side. The VEPTR on the left side continued to migrate and start to come off the rib. Kylies doctors tried to attach a growth rod and move the left side off the rib and over to the area of her spine that had been fused. They were unable too, they didn’t have the right size of connector, so they re-implanted it back on the rib in a different spot. A week later the bulge was coming back more and more each day. By the end of the week, the left VEPTR had come off once again. October 1, 2007, she underwent revision surgery again. This time her doctor had the right connectors. He removed the left VEPTR, connected a growth rod to the part of the device that is attached to the pelvis, attached it over to the bottom of the rod that runs along the fused area of her spine.
So far, things seem to be working! She is scheduled for a VEPTR/Growth Rod expansion in April 2008.
Kylie’s doctors have done so much for her. There are so many doctors out there who would have never of done half of what these two have done for her. They are both determined to do whatever they need to do to allow her to get the growth she needs, before she undergoes a full spinal fusion.
We’re not sure what the future will bring for Kylie, she is fighter. She has overcome so much in her ten years of life. I have no doubts in my mind that she will continue to successfully overcome what ever life throws her way!
She is our precious little angel!!!
Thank you for reading Kylie’s story. We will keep you updated. Feel free to e-mail me at Nlether@yahoo.com with any questions regarding Kylie’s story.
Hadley was born in May 2007. She was born perfectly healthy. Around the age of 5 months, I (mom) saw that one side of Hadley’s ribs were bulging out. I showed my husband, and he thought she just had more muscle strength on that side from learning to sit. Hadley’s head also tilted to one side, and we were told she had torticollis. We were not overly concerned with this diagnosis, since our other daughter also had this. At Hadley’s 6 month appt., my husband thought we should show the doctor Hadley’s back to make sure everything was normal. The doctor looked at it and agreed that Hadley’s ribs were bulging out on one side and she referred us to the local Children’s Hospital.
At 6 ½ months we got Hadley into the Children’s Hospital to see a pediatric orthopedic surgeon. They took an X-ray and that day Hadley was diagnosed with idiopathic infantile scoliosis with a 30 degree curve. The doctor explained to us that most children’s spine’s will straighten up on their own, but there is a percentage of children who have progressive scoliosis. He said he wanted to wait 3 months to see what Hadley’s back was going to do. Not knowing anything about scoliosis, my husband and I agreed to this.
3 months passed and we went back to get more X-rays of Hadley’s back. They looked horrible! Hadley (now age 9 months) had a 55 degree curve. That day she was fitted to get a Kalibus brace. We thought that this brace would correct Hadley’s back within a year or so and scoliosis would be out of our lives forever. At 10 months, Hadley finally got her brace. She had to wear it 24 hrs a day. The only reason we got to take it off was for bath time. Once Hadley got her brace, I decided to do some research on it. I was desperate to find any information on this brace. Unfortunately, I could not find any published research that could prove that bracing could correct scoliosis in an infant. But after praying and searching, I came across the, “Infantile Scoliosis Outreach Program” (ISOP) website. I searched the site high and low for kids using braces, but I could not find any. I saw however, that many of the children on this site were in casts. Even though Hadley was in a brace, I decided to join the “CAST Support Group” because I was desperate for any information or anybody to talk to who knew what we were dealing with. Once I started talking to people on the site, I stumbled across other parents that had personal experience with Early Treatment with EDF (elongation, derotation, flexion) casting, bracing, and other treatment modalities.
People on the “CAST Support Group” welcomed me nicely and showed interest in my situation. I was starting to hear that a lot of their situations sounded similar to ours. They informed me of a new procedure called Early Treatment EDF Casting, which was to try and correct a child’s spine, not just hold it. I was never told that Hadleys brace would not correct her spine. I started to get scared and talked to my husband about what I was hearing. He called Hadley’s orthopedic nurse to clarify the purpose of the brace. Turns out, everything I was hearing on the CAST Support Group was right. A brace was not going to correct Hadley’s back, it was only an attempt to hold it until she is old enough to have surgery! We were told by the nurse that hopefully that wouldn’t be until maybe age 12 or 13; whenever she hits puberty. We were shocked and devastated! This is the last thing we would want for our child. Ineffective bracing until premature surgery! People on the support group informed me of the nearest Early Treatment Center of Excellence, which is the Shriners Hospital for Children in Chicago. So, I immediately called them to try to get Hadley an appt. I was told we had to fill out an application and that it takes approximately 3 weeks to get accepted. Thankfully for God’s guidance and the Cast Support Group, I was able to get advice on how to navigate through the frustrating medical system and we were able to get Hadley an appointment for the following week.
At 11 Months old, we took Hadley to the Shriners in Chicago for a 2nd opinion. This is when we found out Hadley’s back had progressed to 74 degrees while wearing the brace! My research indicated that internal organs could be compromised at approximately 75 degrees, depending on the child…. It was God’s control that led us to the right place before Hadley had permanent damage. The surgeon strongly recommended getting Hadley casted the next day. We agreed to it. We spent the night in the hotel in fear, yet still had hope for Hadley’s back.
The next day, we arrived at the hospital at 6 a.m. to get Hadley casted. We were very scared to have our little baby anesthetized, but knew this is what was best for her. 45 minutes after Hadley was in the operating room, the surgeon came out to inform us that Hadley did very well and was waking up in the recovery room. With the correct casting frame and a solid understanding on the principles of the Early Treatment Process, he was able to get her spine down to a 17 degree curve in her first EDF cast, which was remarkable. We are even more hopeful because Hadley is so flexible. It took a little while to adjust to the cast, but Hadley did very well. I thought not being able to bathe her and let her play in the sand and water would be pure torture, but it wasn’t. She didn’t seem to mind at all. The cast became a part of her life and she is passing all milestones on time.
We were informed that any child with a curve over 50 degrees will more than likely end up needing surgery in the long run, but we are very hopeful. In the back of my head I have always thought, if we had just found a surgeon trained in this gentle, corrective method from the beginning, the chances of Hadley being corrected completely and permanently from the cast would have been so much greater. However, the first doctor that saw my daughter practiced the “wait and see” approach to treatment and in that time her spine progressed 50 degrees! I am just so thankful to have found ISOP when we did, before her spine got any worse.
After 4 weeks of Hadley being in her cast, we went back to Chicago for a follow up appointment. Her X-ray showed that Hadley s spine was at 27 degrees (in cast). It had relaxed a bit, but that’s normal. Then after 2 ½ months of being in that cast, we went back to get it removed and had her 2nd cast reapplied. The surgeon came out to inform us of the correction achieved from the first properly applied EDF cast. He was very pleased with the correction. In Hadley’s first cast, her spine went from 74 degrees to 47 degrees (out of cast). She had 27 degrees of correction. This was phenomenal. The team at the Shriners Hospital for Children in Chicago had done wonders for our baby girl, what more could we ask for!
Hadley stayed in her 2nd cast for about 2 months and then got it changed. From her 2nd cast, she had 8 degrees of correction. We were going in the right direction. Her back was now at 39 degrees. In Hadley’s 3rd cast, she was down to 0-5 degrees(in cast) and the correction from her 3rd cast was 6 degrees. Hadley’s back is now at an miraculous 33 degrees(out of cast).
So far, with God’s help, we are beating the statistics that say anything over 50 degrees can not be corrected from a cast. We pray that Hadley’s spine will continue to get lower in degrees and eventually grow straight from the continual guidance of the EDF serial casting. We hope to avoid surgery, but if it is needed, we are so thankful for Early Treatment with EDF casting, which has the ability to buy my toddler invaluable growing time for her chest cavity until she is older for a more definitive spinal surgery.
Hadley is now in her 4th cast with a 12 degree curve(in cast). She will get her 5th in January. While in the cast, Hadley has learned to do everything any normal child could do, but maybe a little bit differently. Hadley developed a hop when she crawled in order to get places. This helped her when she crawled because she could not bend her legs at the normal crawl position. Hadley has recently learned to walk in her cast as well. It took her a little bit longer to master her balance, but she has accomplished this and is walking every where now.
We are so thankful for Dr. Mehta and ISOP with their Early Treatment Awareness Campaign. It is Dr. Mehta, ISOP, the parents on the CAST Support Group, and the pediatric orthopedic surgeons who are practicing this gentle cure that are helping to make this treatment more widely available in the U.S. and around the world. Without this casting, our toddler would have already had premature spinal fusion/hardware. We are grateful that Hadley may get to avoid repeated and invasive spinal surgeries on her growing spine. Thank you, Dr. Mehta and ISOP for sharing this life saving treatment with parents and the medical community. And Thank you, God for staying at our side and being in control of this situation. Without you, Hadley would not be able to beat the statistics saying anything above 50 degrees needs surgery and would not have been corrected 41 degrees in only 6 months!
After 5 years of trying to have a baby, God blessed us with twin boys. My pregnancy was full of uneasy feelings and lots of “what ifs”. There were many complications along with 3 months of bed rest. After the danger point passed, the doctors sent me home. One week after being home I went into labor.
Ryan and his fraternal twin brother, Matthew, were born in April 2005. They were born 4 weeks early, both were healthy. Our boys came home 2 days later.
The boys were about 2-3 weeks old when my mother noticed Ryan’s ribs felt funny. My mother-in-law had made comments about it as well. Not knowing anything about Infantile Scoliosis, I thought this was due to them still being small babies. As Ryan grew, we noticed he always leaned his head to one side. We now know he had torticollis. It was never treated and he slowly outgrew it.
While bathing the boys, around 7 months old, I noticed Ryan’s back protruded on one side. I still knew nothing, but wondered often if something was wrong. At his 9-month check-up, we pointed it out to his pediatrician. She immediately told us she felt he may have Infantile Scoliosis. We had heard of teenage girls having scoliosis, but had no idea babies could have scoliosis. It was a weird feeling not knowing. She referred us to Texas Scottish Rite Hospital for Children in Dallas, Texas. Shortly after the pediatrician’s referral, Ryan was diagnosed with Progressive Infantile Scoliosis. X-rays showed a 29 degree right thoracic curve. They recommended a CT Scan and MRI to rule out any congenital abnormalities. They also wanted us to see a geneticist. We were told they would watch him closely and wanted to see him back in 3 months. At that time, his doctor also talked in-length about Early Treatment with casting. We were stunned and confused, but knew we wanted to avoid surgery if at all possible. If Ryan’s curve continued to progress, casting sounded like the best treatment for him.
In 3 months time, Ryan’s curve had progressed from 29 to 34 degrees. We then knew casting was what Ryan needed, and it would be in our very near future. Ryan still, however, needed the MRI. He and his brother were constantly sick so we had to continuously put this procedure off. Ryan was finally well enough for the MRI and thank God it came back normal. We saw the geneticist and she felt his scoliosis was mainly “positional” while in untero. The geneticist did not think there was an underlying syndrome diagnosis.
The procedures were all done and all came back normal, so the date was set for Ryan’s first cast. He was 15 months old (still a baby), had just started walking and I was SCARED to death. A cast?! A hard cast? No baths, no playing in water. He is going to stink! How will he sleep?! He will not be able to do all the things his twin brother will do! My mind was going crazy with all these bad thoughts of a cast. I needed to talk to someone else who had been through the same thing.
Days before his first cast was applied, I found ISOP on the internet. How had I missed it all those times I was searching for answers and information? I was still so scared and had no idea what I might learn, but ISOP had a support group. I wasted no more time. I immediately joined the group.
Fast forward to November 2008…………Ryan is now in a brace ONLY at night!!!!! He was in a series of 6 casts over 14 months. And wore his brace 23 hours a day for 10 months. Today his curve is down to 8 degrees and he looks GREAT!!!
Casting was nothing like I thought it would be. Within a week Ryan was walking again just fine. His baths? Well, we came up with other fun bath ideas. Playing in the water was just a special treat for the boys when his cast was removed the day before the new one was applied.……..they didn’t miss a thing. Stinking….we just didn’t have that problem. And he slept……like a baby, within a week of his first cast.
Ryan adjusted so well to the cast and didn’t miss a beat. He did everything his twin brother did and more! Looking back, I only wish I would have known about Early Treatment sooner. Ryan would have been in casts very early on. Casting is a gentle method for treating Infantile Scoliosis. And, for most babies, if treated early and properly, has the ability to train their young spines to grow straight, gently and permanently and surgery is not needed.
We are so informed about Infantile Scoliosis because of ISOP and the CAST support group. I have learned more here, and through the support group than what any doctor could have told me. The support group is a God send. I don’t know how I would have made it through without communicating with other Moms and Dads going through the same thing.
If you are just discovering your baby/child has Infantile Scoliosis, join the group. It has a wealth of information for you and allows interaction with other parents who are experiencing the same situations. I cannot thank ISOP and Dr. Mehta enough for all they have done to educate us about Ryan’s condition.
Ryan will go in a few weeks for a check-up and we are in hopes he will be finished with the brace.
Early Treatment with EDF (elongation, derogation, flexion) casting works.
If you have any questions about Ryan’s treatment feel free to email me. Ryanswalk@yahoo.com
To view a blog dedicated to Ryan and others with infantile scoliosis go Here.
Our daughter Bridget was born on the 22.2.01. She is the fourth child in our family and her two brothers and one sister were over the moon at having a new addition to the family.
Bridget spent her first year drowning in the attention of her siblings. She sat on her own at about 8 months and it was at this time that I noticed she seemed to sit more on her left buttock. Looking back at photos she also had her head turned to the right in most photos though I did not pick that up at the time. When she was viewed from the back while sitting, it looked as though her spine curved towards the left side.
At 10 months I took her to our GP and then to a paediatrician. The paediatrician said the curve was an optical illusion and not worth xraying. I left the consultation relieved but continued to watch her spine as she was sitting or in the bath. At 16 months Bridget was still not walking. She had developed a bottom shuffling technique which involved leaning to the left and using her left hand behind her and her right hand at the front to propel herself quite quickly around the floor.
I returned to the paediatrician when Bridget was about 18 months. She was still bottom shuffling and when sitting had creases visible on one side of her waist. I pointed this out to the paediatrician but she said she could have built up muscles on one side of her body from bottom shuffling. She felt the curve was an illusion created by her posture and advised me not to be concerned about it.
Bridget finally walked at 22 months. As she progressed from the first toddling steps to competent walking and running her gait remained uneven. She seemed to weight bare more on the left leg and her right shoulder was lower than her left. When standing and in swimming togs we could clearly see a curve in her spine.
I returned to our GP when Bridget was almost three. I showed him the curve in her spine and he agreed with me that it was unusual. He referred me to another paediatrician. This paediatrician felt there was nothing to worry about as he believed her apparent curve was postural and told me we could xray if I liked but he wouldn’t foresee any need for intervention.
The xray revealed a 38 degree thoracolumbar curve. We were referred to a spinal surgeon who arranged for her to have an MRI as he felt sure there must be some neurological problem which was contributing to her scoliosis. This doctor explained that while she was under anaesthetic she would be cast for a TLSO brace.
The MRI and a subsequent consultation with a paediatric neurologist could find no neuromuscular involvement and with no vertebral abnormalities present, Bridget’s curve appeared to be Infantile Idiopathic.
Six weeks later we returned to the Spinal Surgeon to learn about Bridget’s brace. He told us that the brace would not correct the curve nor stop its progression and he estimated by the time Bridget was 10 years old the curve would be so large and the resultant deformity so disfiguring that he would be operating to fuse her spine though she would be far from skeletally mature. He said without the brace the curve would progress much more quickly and he estimated he would be fusing her spine at 7. He explained that as the spine could not grow at the fused area this would result in her having a short trunk and long arms and legs like a “daddy long legs spider.”
Our family was horrified by this prognosis. We sought the opinion of another spinal surgeon in Brisbane as well as consulting with two others in Sydney and Melbourne. Each emphasised how rare Infantile Idiopathic Scoliosis is and mentioned that it was more prevalent in the UK.
I understood that the treatment Bridget was receiving was the standard treatment in Australia but was keen to research how Infantile Idiopathic Scoliosis was treated in other countries. I started with the UK. The Scoliosis Association of the UK website www.sauk.org.uk explained how Infantile Scoliosis could be corrected if treated early enough with a series of plaster casts. I gleaned this information from the SAUK site as it was in 2004. I notice that it has since changed and no longer mentions infantile scoliosis as a separate and curable condition using serial plaster casts.
To apply these casts the child is anaesthetised and suspended on a paediatric traction table. The spine is gently manipulated and placed in a corrected position. The plaster cast is then applied to hold the spine in that position. A widely trimmed mushroom shaped window is left trimmed around the tummy/chest to allow for expansion (chest expamsion window). Another hole is left selectively at the back over the concaved flattened side of the ribs so that the child’s own breathing and laughing encourage symmetrical growth. This alters the direction of the spine and allows it to grow in a straightened position. The cast is changed every three months and the process repeated until the curve has been corrected.
It was emphasized that it is the growth of the spine while it is held in the corrected position that ensures that it stays straight and never needs fusion. For this reason the best and quickest results have been obtained in children under two years as it is at this age that the most rapid rate of growth occurs. All this information I learned from reading the SAUK website as it was at that time and from speaking to Dr Mehta on the phone.
Dr Min Mehta has been successfully using her Early Treatment casting technique in the UK for over 30 years.
I sent Bridget’s xrays to Dr Min Mehta. After viewing Bridget’s xrays and photographs Dr Min Mehta said she believed 18 months of serial plaster casts changed every three months would cure Bridget’s scoliosis but only if treatment was started straight away. She recommended we see a specialist at the Royal National Orthopaedic Hospital in Stanmore, England since she had recently retired from NHS practice.
It was about this time that I read Ella’s Story on the Scoliosis Associan of Australia (SAA) website. I contacted them immediately to see if there was any possibility that serial plaster casting was being used to treat Infantile Scoliosis in Australia. Ella was born in the UK and had since returned to Australia. Ella was casted between 6 months and 14 months by Dr Mehta just before Miss Mehta retired. She is now 13 yrs old and has remained straight. At 6 months Ella had a 60 degree curve. .
In October 2004 we saw the pediatric spine specialist at the RNOH, Stanmore. He applied the first of Bridget’s plaster casts under general anaesthetic. We were delighted to see that in her cast her curve improved from 38 degrees to 21degrees.
Bridget wore her first cast for almost three months. She was a very active and happy child who loved jumping on the trampoline and riding her bike. Wearing a plaster cast did not restrict these activities. On January 9th 2005 we returned to England to have her plaster removed and her second cast applied. At this time I met with Dr Mehta and showed her Bridget’s cast that was applied by the specialist at the hospital from which she recently retired. Miss Mehta was disappointed to see that the specialist was not using the correct mushroom shaped windows to prevent barrel shaped ribs.
At this point, I had made contact with Heather Hyatt, ISOP and the CAST group. I applied to have Bridget included in the first ever ETTP (Early Treatment Trial Project) organized by ISOP at Shriners Salt Lake City. Dr Mehta travelled to SLC to train staff and demonstrate her method of Early Treatment w/ modified EDF casting using a group of patients who were lucky enough to be the first to be treated with this method in the USA. We were very fortunate to have Bridget accepted into this group in May 2005.
Bridget had 14 months of casts from aged 3 yrs 7 months to 4 yrs 9 months. During that time her curve went from 38 degrees to 8 degrees in cast but her curve would go back to 25 degrees out of cast. The casts totally got rid of her rotation and rib hump. At this time she was diagnosed with a connective tissue disorder,
At this point with the Doctors and physios talking together we decided to change to a brace and combine aggressive bracing with an exercise (core strength) program and posture training.
For the last 8 years we have travelled to Salt Lake City every 6 months to have custom fitted braces and shoe orthotics made for Bridget. (who also has a leg length difference) She currently has a providence brace for night time and a modified Boston brace based on the Mehta style Cast with same mushroom shaped window at the front.
Bridget is now almost 12 and a half. She is 155cm tall and enjoys swimming, playing netball and the same active life as any 12 year old. She still has a double curve which has increased over the years (52 thoracic and 42 lumbar) but we are hoping to avoid surgery (fingers crossed) depending how much growing she has left and what her curves do. At the moment, thanks to the hard work of Drs and physios over the years she has no pain, minimal deformity and a wonderful quality of life.
I would dearly have loved the opportunity to cast under 2 when we had the best chance of achieving a permanent cure like Ella in England and the 100s of kids now cured in the USA thanks to Dr Mehta’s treatment.
Guardianship is a court appointment which gives a person or an organization responsibility and authority for making decisions on behalf of an adult who is unable to manage his/her own affairs and make his/her own decisions. Guardianship for adults in Colorado is authorized by Colorado Revised Statutes, Title 15, Article 14, Part 3. The person for whom a guardian is appointed is called a “ward.” Guardianship is a serious responsibility and one that should be approached with the same seriousness and attention which you apply to your own life. Besides being a “legal representative” for your ward, you will also be an advocate and watchdog. You may also be a surrogate family member, teacher and a friend. While guardianship provides important protection and assistance, it is also very restrictive. It can remove all of a person’s legal rights to manage his/her own life and must be imposed only as a last resort.
If you are considering becoming a guardian for someone you must first consider if limited guardianship would be sufficient. Colorado law presumes that only limited guardianship is necessary and you must prove to the court otherwise if an unlimited guardianship is requested. Limited guardianship may include authority to make only medical decisions, only residential decisions, or only financial decisions. Or it may include a combination of one or two areas. In all other matters, the guardian has no authority. An unlimited guardianship can be reduced to a limited guardianship, or the reverse can be done, through a petition to the court which made the initial guardianship appointment.
Duties of a Guardian
As a guardian you are expected to understand and carry out the responsibilities outlined in the specific guardianship orders of your appointment. When in doubt about your authority to decide about a specific matter, you may always seek prior approval from the court. While individual guardianship orders may contain specific instructions, there are general duties and responsibilities which every guardian is expected to fulfill.
Colorado law gives guardians authority to make decisions regarding the ward’s support, care, education, health, and welfare.It further states:
“A guardian shall exercise authority only as necessitated by the ward’s limitations and, to the extent possible, shall encourage the ward to participate in decisions, act on the ward’s own behalf, and develop or regain the capacity to manage the ward’s personal affairs. A guardian, in making decisions, shall consider the expressed desires and personal values of the ward to the extent known to the guardian. A guardian, at all times, shall act in the ward’s best interest and exercise reasonable care, diligence, and prudence.” (C.R.S. 15-14-314(1))
In addition, a guardian shall:
Become or remain personally acquainted with the ward and maintain sufficient contact to know of the ward’s capacities, limitations, needs, opportunities, and physical and mental health. (C.R.S. 15-14-314(2)(a))
Take reasonable care of the ward’s personal effects and bring protective proceedings if necessary to protect the property of the ward. (C.R.S. 15-14-314(2)(b))
Spend the ward’s money that is in the guardian’s control, for the ward’s current needs for support, care, education, health, and welfare. (C.R.S. 15-14-314(2)(c))
Save any of the ward’s excess money for the ward’s future needs. If a conservator is appointed for the ward, the guardian must pay the excess money to the conservator, at least quarterly, to be saved for the ward’s future needs. (C.R.S. 15-14-314(2)(d))If your ward has substantial assets (more than the amount required for his/her daily living needs), it is necessary that a conservator be appointed. A conservator is a person or organization appointed by the court to manage the financial affairs of another. The process for appointment of a conservator is similar to that for a guardian. If your ward is also your relative, it may be possible for you to serve as both the guardian and conservator.
Immediately notify the court if the ward’s condition has changed to the degree that guardianship may no longer be necessary.
Inform the court of any change in the ward’s residence.
Immediately notify the court of the ward’s death.
Powers of a Guardian
Unless limited by the court order, guardians have the following powers:
Consent to medical or other care, treatment, or service for the ward. (C.R.S. 15-14-315(1)(d))Advance Directives are arrangements and desires which your ward may have expressed in writing while competent. The Living Will is an example of such an advance directive regarding withholding or withdrawing medical life support systems and/or nourishment. You are obligated to respect your ward’s wishes and directions contained in the Living Will.Another Advance Directive is a Medical Durable Power of Attorney with which your ward would have designated an agent who is to be responsible for making such decisions on his/her behalf. The agent specified to make decisions on your ward’s behalf in the Medical Durable Power of Attorney, has precedence for making health-care decisions over a guardian unless the Medical Durable Power of Attorney is revoked by the court. A guardian may not revoke the ward’s Medical Durable Power of Attorney. (C.R.S. 15-14-316(3))
Apply for and receive money payable to the ward, guardian or custodian for the support of the ward from any government or private source. (C.R.S. 15-14-315(1)(a))
If not in conflict with other court orders, the guardian may take custody of the ward and decide where the ward is to live. Guardians must obtain permission from the court to move the ward outside of the State of Colorado. (C.R.S. 15-14-315(1)(b))
If there is no conservator, the guardian may take necessary actions to force an obligated party to support the ward or to pay money for the benefit of the ward. (C.R.S. 15-14-315(1)(c))
Depending upon circumstances, a guardian may allow a ward to make certain decisions affecting the ward’s well-being. (C.R.S. 15-14-315(1)(e))
With specific authority or direction from the court, a guardian may consent to the adoption or marriage of the ward. (C.R.S. 15-14-315(2))
A guardian may petition the court for authority to apply for a divorce or legal separation on behalf of the ward if it is in the best interest of the ward based on evidence of abandonment, abuse, exploitation, or other compelling circumstances, and the ward either is incapable of consenting or has consented . (C.R.S. 15-14-315.5)
Rights, Immunities, and Limitations
With approval by the court, guardians are entitled to reasonable compensation for services as a guardian and to reimbursement for room and board provided by the guardian or one affiliated with the guardian. If there is a conservator, other than the guardian or one affiliated with the guardian, reasonable compensation and reimbursement to the guardian may be paid by the conservator without order of the court.
Guardians are not required to provide for their ward, or pay for their ward’s expenses, out of the guardian’s own funds. However, you must very carefully read all documents before signing. If you sign something personally accepting financial liability, you may be held personally liable. Neither are guardians liable to third parties for acts of the ward solely by reason of the guardianship. Further, a guardian who exercises reasonable care in selecting parties to provide medical or other care, treatment, or service for the ward, is not liable for injury to the ward resulting from the negligent or wrongful conduct of the providers.
Guardians may not consent to involuntary commitment, or care and treatment of a ward for mental illness, developmental disabilities, or for alcoholism or substance abuse. In all of these instances, a guardian must proceed under the appropriate statute.
Reports to the Court
Within 60 days of appointment, or as otherwise directed by the court, guardians must submit a written report to the court including:
the condition of the ward,
the guardian’s personal care plan for the ward, and
account for money and other assets in the guardian’s possession or control.
Thereafter, guardians are required to submit annual reports which cover:
the current mental, physical, and social condition of the ward;
the ward’s living arrangements;
medical, educational and vocational services provided and the adequacy of the ward’s care;
a summary of the guardian’s visits with the ward and actions on behalf of the ward, including the ward’s participation in decision-making;
whether the current care plan is in the ward’s best interest;
plans for future care; and
recommendation as to continued need for guardianship and changes.
In addition, the court may appoint a visitor to review a report, interview the ward or guardian, and make any other investigation the court directs.
General Responsibilities
As a guardian you must know and care about all aspects of the well-being of your ward. If he or she does not live with you, you must visit and spend time with him/her as often as possible. It is your responsibility to make arrangements for, keep informed about, and maintain documentation of your ward’s current situation regarding finances, living arrangements and care givers, health and medical care, education and training, personal needs, preferences and desires, employment, recreation and leisure time.
It is very important to get acquainted with the people who are significant in your ward’s life, for example, family, doctors, nurses, recreation directors, case workers, employers, therapists, teachers, friends, and neighbors.
You are expected to plan for your ward’s future. Anticipate and be prepared for emergencies. Be aware of options in living arrangements or daily living activities in case changes might be necessary. Make sure that insurance or appropriate health care benefits are in place. Assure that funeral and burial or cremation arrangements are in place.
It is important for you to be familiar with laws, rules and regulations that may impact the life of your ward. For example, laws and regulations regarding nursing homes or other residential facilities; laws against discrimination and safety requirements if your ward is employable; education laws if he/she is under age 21; any government benefits and entitlements that he/she might be eligible to receive. You will also need to know how to advocate for your ward in these matters. There are community resources available to provide help, information and assistance.
Making Decisions on Behalf of Someone Else
Even though, as a guardian you will have responsibility for protecting and caring for your ward, it is important to carefully distinguish between providing adequate protection and imposing excessive restrictions. As has already been stated, Colorado law requires guardians to include their wards in making decisions. A ward’s ability to participate will depend to a large extent upon the magnitude of the decision. For example, what to wear to a particular event is a much easier decision than whether or not to have surgery. The kind of information and how it is presented will also have a bearing upon the ward’s ability to participate in a decision. Information should be tailored to the understanding of the individual; the language must be simple, repetition may be necessary, and visual aids may be helpful. Following the attempt to inform, special efforts should be made to determine whether the person has in fact understood the information, perhaps through quizzing or other feedback. You may also enlist the help of others to explain a matter to your ward, possibly in a different setting and at a different time of day.
As a guardian you must weigh all decisions critically and objectively. The following guidelines may be helpful. First, allow your ward to make the decision alone with support and assistance only as needed. If that is not possible, include your ward in a decision-making process whereby all relevant information is discussed and your ward is an active participant. Finally, if a decision must be made by you alone, you must be sensitive to the expressed preferences of your ward, if known, and to the greatest extent possible, make decisions based upon the same set of values he/she would use if making his/her own decisions. In the case of a ward who has never been able to make his/her own preferences known, you have no choice but to make the decision that you believe is best for your ward.
When making decisions for your ward, you must apply informed consent principles in the same manner applied when making decisions about your own life. For example, before giving consent you should have answers to the following questions:
What are the alternatives?
What are the risks?
What are the benefits?
What are the consequences?
What discomforts might occur?
Can I change my mind later?
Termination or Modification of a Guardianship
A guardianship terminates upon death of the ward, or if the ward no longer meets the standard for establishing the guardianship. (Incapacity by clear and convincing evidence.) A ward, guardian or any interested person may petition for removal of a guardian on the grounds that removal would be in the best interest of the ward or for other good cause. Before terminating a guardianship, the court will follow the same procedures to safeguard the rights of the ward as apply to a petition for guardianship. The court may remove a guardian or permit a guardian to resign. A petition for removal or permission to resign may include a request for appointment of a successor guardian. (C.R.S. 15-14-112 and 318)
The court may modify the type of appointment or powers originally granted to the guardian if the extent of protection or assistance is currently excessive or insufficient or the ward’s capacity to provide for support, care, education, health, and welfare has so changed. (C.R.S. 15-14-318(2))
A temporary substitute guardian may be appointed for up to six months when a guardian is not performing effectively and the ward’s welfare requires. (C.R.S. 15-14-313) Except as otherwise ordered by the court, a temporary substitute guardian has the same powers as the original guardian.
Delegation of Power by a Guardian
By the use of a power of attorney, a guardian may delegate to another person, for a period not exceeding 12 months, any power regarding care, custody, or property of a ward, except the power to consent to marriage or adoption. This provision is useful if a guardian must be out of the geographical area for an extended period or during a medical leave. (C.R.S. 15-14-105)
Transfer to another country or state
The court making the appointment of a guardian may transfer the guardianship to a court in another county or another state if the court is satisfied that a transfer will serve the best interest of the ward. (C.R.S. 15-14-107(1))
For more information please call 303-228-5382, or send an email.
Living Will- Declaration Concerning Medical or Surgical Treatment
Can only be set up while a person is competent to understand the consequences of the decisions.
In order for a Living Will to become operative, four conditions must exist:
The individual (the declarant who has signed the Declaration) must be terminally ill due to an incurable or irreversible condition.
The individual must be unable to decide whether to accept or reject medical or surgical treatment.
The individual must be unable to make that decision because of unconsciousness or incompetence.
The individual, or one acting for the individual, must submit the Declaration to the physician for entry into the individual’s medical record.
When these required conditions exist, the attending and one additional physician must:
Certify the individual’s terminal condition in writing on the hospital record.
Immediately attempt to notify the individual’s spouse, any adult child, parent or agent under a Medical Durable Power of Attorney (in that order) of the certification.
After the physicians’ certification is made, a period of 48 consecutive hours is granted by law for a challenge to the validity of the Declaration.
A parent, adult child, spouse or MDPOA agent may challenge the Declaration in the district court in the county in which the patient is located.
A legal representative is appointed for the patient and notice is given to certain adult relatives.
The court determines the validity of the Declaration.
A physician, or a hospital or person acting at the physician’s direction, is free of criminal or civil liability for acting in accordance with a valid Declaration.
In certain situations, the law allows the physician to take actions not specifically provided in the Declaration:
If the declarant is pregnant and if life-sustaining measures would enable the fetus to develop and survive, the Declaration is not enforceable.
If pain results from the discontinuance of artificial nourishment, the physician may order that nourishment be provided to alleviate the pain.
A Declaration does not have to be notarized, but must be witnessed by two witnesses. Said witness shall not be:
The attending physician or any other physician; or
An employee of the attending physician or health care facility in which the declarant is a patient; or
A person who has a claim against any portion of the estate of the declarant at his death at the time the declaration is signed; or
A person who knows or believes that he is entitled to any portion of the estate of the declarant upon his death either as a beneficiary of a will in existence at the time the declaration is signed or as an heir at law.
If the declarant is a patient or resident of a health care facility, the witnesses shall not be patients of that facility.
In the event that the declarant is physically unable to sign the Declaration, it may be signed by some other person in the declarant’s presence and at his direction. Such other persons shall not be any of those listed in Paragraph 7 above.
A Declaration may be revoked by the declarant orally, in writing or by burning, tearing, canceling, obliterating or destroying such declaration.
Forms are available from hospitals, medical societies, the Guardianship Alliance and most stationery supply stores.
It is wise to have both a Medical Durable Power of Attorney and a Living Will. The Medical Durable Power of Attorney gives someone (an agent) authority to make decisions; the Living Will sets forth one’s desires regarding life sustaining treatment and gives direction to the agent under the Medical Durable Power of Attorney.
Durable Powers of Attorney
With a Power of Attorney, a person (the Principal) appoints another person or organization (the Agent or Attorney-in-fact) to act on his/her behalf in all matters as designated in the document. A person (the Principal) must have capacity to understand the consequences of the document.
In Colorado, there are two Durable Powers of Attorney:
Medical Durable Power of Attorney includes medical and personal decision-making authority which may be limited or broad.
General or Financial Durable Power of Attorney includes decisions about money and property and can include other matters, except medical decisions.
“Durable” means the agency continues if the principal becomes incapacitated. To be durable the document must contain wording such as “this power of attorney shall not be affected by the subsequent incapacity or disability of the principal.
A principal may revoke any power of attorney at any time even if he/she is considered to be incapacitated by a doctor, caregiver or family. To make changes in a document, he/she must write a new one.
An agent may not override the principal’s wishes even though the principal may be assessed as incapacitated.“Nothing in this section or in a medical durable power of attorney shall be construed to abrogate or limit any rights of the principal, including the right to revoke an agent’s authority or the right to consent to or refuse any proposed medical treatment, and no agent may consent to or refuse medical treatment for a principal over the principal’s objection.” C.R.S. 15-14-506.(4)(a)
An agent has the same authority for medical treatment as a guardian. If another person is appointed as the guardian for the principal, the agent has priority for making medical treatment decisions unless the Power of Attorney is revoked by the court.
An agent is obligated to follow the principal’s instructions when making decisions. Unless the DPOA states otherwise, the agent has the same authority to make decisions which the principal would make if able to do so.
The appointment of a spouse as an agent dissolves on divorce.
It is a good idea to designate a successor agent in the event an agent is unwilling, unable, or ineligible to act when a decision is necessary. A successor agent has the same authority as the primary agent.
Powers of Attorney can be set up through an attorney knowledgeable about estate planning and health care issues or set up with preprinted forms which are available from hospitals, nursing homes, or the Guardianship Alliance.
Colorado law does not require a DPOA to be witnessed, however, it is recommended that there be two witnesses or have the document notarized.
For more information please call 303-228-5382, or send an email.
Unfortunately, at this time, scoliosis checks are not part of the suggested guidelines for Well Baby Checks. While pediatricians and family physicians provide a general look at your baby’s overall health, it may fall on your shoulders to monitor this. One of the best tools that you have is your camera. When you suspect that your child’s spinal growth is not normal, take pictures of your baby’s back on a weekly basis to monitor and compare through time.
Your parental intuition will make sure that your baby has the best options for his or her health. Follow your gut!
MGGC is a gentle, conservative, and perhaps most importantly, non-invasive treatment option to
address the three dimensional curves of progressive infantile scoliosis. There are no side effects when MGGC protocols are applied by a surgeon who has received proper, specialized
training.
In contrast, the complication rates for surgery and implantation of distraction hardware involve numerous risks and complications, including:
Rod breakage inside the body
Premature spinal fusion
Risk of infection
Potential for chest wall rigidity
Also, a study of 38 patients treated with dual growing rods demonstrates that the gains from lengthening decreases with each subsequent lengthening and over time. Cobb angle improves after the initial instrumentation but does not change significantly with repeated lengthenings. Spine May, 2011
ISOP advocates that conservative treatment with MGGC is a first line of defense, and that in most cases, surgery is a last resort.
Back to Frequently Asked Questions for Parents
Mehta’s Growth Guidance Casting (MGGC) is a validated, non-surgical, potentially
curative treatment for progressive infantile scoliosis (PIS). PIS in infancy is considered the only potentially life threatening condition in the world of pediatric orthopedics because the curve(s) will keep pace at the rate of the child’s growth, which is fast the first two years of life.
Scoliosis is a three-dimensional issue which can be addressed gently in all dimensions with this specialized EDF (Elongation, Derotation, Flexion) treatment. Early Treatment with MGGC involves application of specialized plaster casts on a specially-designed frame. The number of casts needed will be determined as the curve is measured over time by your child’s physician.
The modified “under arm” casts were developed by American surgeons and were never included in Mehta Casting protocols. Under arm casts only have the ability to address curves below T-8. It is worth repeating that over the shoulder casts address all curve types at all locations.
Mehta casts must be applied by a trained pediatric orthopedic surgeon. The child is under anesthetized and placed on a pediatric size EDF casting frame. For more information about the frames required, please visit www.noeledfcastframe.com.
Back to Frequently Asked Questions for Parents
Early Diagnosis and Early Treatment are the core of successful treatment with Mehta’s Growth Guidance Casting (MGGC) for one simple reason.
The human body grows at an unbelievably rapid rate during the first two years of life. This growth rate will never be experienced again during human development, and it acts as the corrective force that allows spines affected with progressive infantile scoliosis (PIS) to actually grow straight three dimensionally. MGGC casts address spinal curves in terms of elongation, derotation and flexion.
The mushroom-shaped window that identifies a Mehta cast is a vital key to your baby’s future health because:
It allows them to breathe normally and fully
It accommodates their developing heart, lungs and internal organs
The human body grows at an incredibly rapid rate during the first two years of life and MGGC casts are meant to work WITH this growth, never to impede it!
The widely trimmed, mushroom-shaped window is a chest expansion window that prevents chest wall
deformities caused by Risser style casts. Ribs are flexible prior to the age of two, and the rib flaps of this important opening prevent permanent rib flaring.
Back to Frequently Asked Questions for Parents
MGGC is a gentle, conservative, and perhaps most importantly, non-invasive treatment option to
address the three dimensional curves of progressive infantile scoliosis. There are no side effects or
lingering complications when MGGC protocols are applied by a surgeon who has received specialized
training.
This sharply contrasts the complication rates for surgery and implantation of distraction hardware (rods,
etc), which requires numerous and repeated surgeries and involves a complication rate that is quite
high. It is important to keep in mind that these are babies and they are experiencing the rapid growth
that sets up their future health and life. Surgery is the last resort, not the first.
Back to Frequently Asked Questions for Parents
As a nonprofit program, ISOP dedicates its resources to families affected by progressive
infantile scoliosis (PIS), training physicians in the Early Treatment Protocol and growing the availability of MGGC worldwide. This is possible thanks to your donations and the generosity of ISOP sponsors.
While all physician’s are familiar with the basics of casts and casting, Mehta’s Growth Guidance Casting
(MGGC) is a specialized procedure that requires a specific type of frame and a surgeon who has been
trained in the protocol. Your child’s surgeon may not be familiar with MGGC. Please refer her or him to
ISOP’s website for resources and access to specialized training.
Back to Frequently Asked Questions for Parents
Once it is determined that your child has scoliosis, determining the exact type is next. There are several types of scoliosis that affect infants.
Progressive Infantile Scoliosis
Diagnosed from birth to age 2
Considered a non-structural type of scoliosis
Congenital Scoliosis
A structural issue of the vertebrae present at birth
Examples are hemivertebrae, chiari malformation, syringomeyelia, tethered cord
By definition, progressive scoliosis will not resolve without medical intervention, so watching and waiting could result in permanent changes to your child’s spine. Early Treatment is vital because your baby is growing so quickly.
Back to Frequently Asked Questions for Parents
Early Diagnosis and Early Treatment are at the core of successful treatment with Mehta’s Growth
Guidance Casting (MGGC) for one simple reason. The human body grows at an unbelievably rapid rate
during the first two years of life. This growth rate will never be experienced again during a human’s
development.
This rapid growth rate is the corrective force that allows spines affected with progressive infantile
scoliosis (PIS) to actually grow straight.
Back to Frequently Asked Questions for Parents
My child would have faced severe deformity or a very early and painful death, if not for the work of the ISOP. Dr. Min Mehta’s method of early treatment for Infantile Scoliosis is directly responsible for saving my son. The ISOP needs funding so that all children diagnosed with this condition can get this life saving treatment.
Thousands of babies and young children around the world currently have this condition, and very few doctors are trained to treat it. This is literally a cure, for the most difficult orthopedic condition to treat in very young children. EDF casting is a non-surgical, safe and inexpensive treatment, but a very small percentage of the medical community even knows it exists. This grant will help get the word out to the medical community, train more doctors, and immediately begin saving babies lives.
My son Max is 18 months old and has infantile idiopathic scoliosis. When he was diagnosed at 3 months and I began my research ISOP was the only place that gave me the information that I needed to begin this journey. My son had been in a brace and was doing very poorly and I needed to know that there were other alternatives out there. Thanks to Heather and the support of ISOP I was able to make a well informed decision that was right for my son and our family.
The articles, information and advice from the other members are just what I needed to mke me feel like I was not alone. Without Heather and ISOP it would be impossible for other families to get the materials that they need to make a well informed decision on their childs care. This is the only place that has the amount of good information on this topic.
We could not be happier with the doctors at Shriners and the care that Max is receiving. Without Heather and ISOP this would be impossible.
Please allow Heather to continue the mission that she has begun and allow her to share this special gift that she has with other families who need the support.
I have to say that if it weren’t for Heather Hyatt-Montoya I’m not sure where we would be today. My son was diagnosed with a 24degree curve at 1yr old that very quickly progressed. The first doctor we saw wanted to watch and wait (which is currently the norm). We were so lost and in the dark because the doctor didn’t really explain anything to us except that our son had scoliosis. When we asked about bracing, casting or even surgery she really couldn’t answer what the future would hold.
I found ISOP’s website and contacted Heather to find out more about the condition and what could be done. If it hadn’t been for her we would have sat and watch our son’s back get worse and would have ended up with surgery in the future. We went for a second opinion with a doctor that had been successful in early treatment for scoliosis using casting. Because we had talked to Heather and knew this doctor was trained and very good we did not hesitate. I am happy today to report that my son had a curve over 40 degrees when we started the early treatment process and after casting and bracing for 2yrs he is staight and doing well. We thank God every day for Heather and our little guys life being saved. I would love to see this happen so that many many more doctors can be trained and that we can continue to raise awareness for early detection of Infantile Scoliosis. Early detection and trained doctors are the key in saving these babies lives so they can live a normal life instead of one full of back surgeries every couple of months to lengthen growing rods.
No one and nowhere else can any of us who are associated with this dreaded affliction, find the information, treatment, and support for our kids. It’s very much like MDA, if it weren’t for Jerry Lewis alot more would suffer horribly. Well, Heather Hyatt-Montoya is our Jerry Lewis. Our kids are “Heather’s Kids”! We are Heather’s partners in this crusade to “fix” the kids without using the previously accepted and debilitating procedures currently in place.
The Mehta method CURES, none of the other processes dare use that term. Getting more professionals/doctors onboard will only and inherently lower the number of beautifully, wonderful children from ever having to suffer such a monstorous future of pain, and possibly death. The Dr. Metha method is like other things in our life, the idea is so simplistic it gets overlooked. It is believed this type of corrective action can’t possibly be effective. Well, we have seen a 50% improvement for our child in just the very first installment of this miracle of science. Our child is on his way to what we know will be a lasting/permanent healthy life because we were able to a part of such a committed group of medical and private individuals.
ISOP literally saved my son, Evan’s life. When we were told to wait and watch our 3 month old sons progressive infantile scoliosis progress, we found ISOP who directed us to a physician practicing early treatment. Within a matter of 8 Mehta casts, my son’s spine is now straight.
I am a firm believer in early treatment, in ISOP and believe the medical community should embrace this gentle, non-surgical treatment as an alternative to invasive surgery.
My family now supports ISOP, and we’ve facilitated several benefits to ensure that other families of children with progressive infantile scoliosis have the same opportunities for treatment/success as we have. ISOP facilitates early treatment seminars across the USA to help educate the medical community and provide treatment information to families in the same situation we were in several years ago.
The founder of the Infantile Scoliosis Outreach Program, Heather Hyatt-Montoya, is the reason that the life saving method of casting is available in the U.S. at all. Dr. Min Mehta’s Early Treatment method is saving my 21 month old baby’s life at this very moment, and we never would’ve found a doctor to help without finding the ISOP website.
Time was running out for my baby, his spine was at a 64 degree curve and rapidly progressing, at only 19 months of age. Had he not been cast in this plaster jacket, he would have likely progressed to a degree of curvature that would’ve crushed his vital organs and even been fatal at a very young age. When I say very young age, I mean before the age of three years old.
Our only other option would’ve been a decade or more of bracing, which often does not stop the dangerous curve from progressing. Bracing would have led to spinal “growth rod” surgery for our baby, at an age as young as two years old. He still could’ve led a lifetime of pain and deformity, even with multiple surgeries.
This is how important the work the ISOP is doing, and there are very few doctors in the U.S. and around the world who are trained in this method, or are even aware that it exists. Parents are desperately searching for help for their babies, and many are not as lucky as us. This is heartbreaking and it is simply unacceptable, when there is an actual known cure for this condition, if caught in time. More doctors must be informed and trained in EDF to save these baby’s lives.
Because of the work of Dr. Mehta and the ISOP, we have a wonderful doctor at a Shriners Hospital, who is already training others as he continues to rescue children. Our child now will not be deformed or die from this condition. Please help us give that gift to those who so desperately need it.
January 3, 2014 – Savanna is a super sweet, super cute 18.5 month old little girl. She will be 19 months when she gets her first cast. Why does she need a cast? She has been diagnosed with Progressive Infantile Scoliosis, and casting is a gentle, non-invasive way to encourage her spine to grow straight.
A little background on Savanna… She was a breech baby. No matter what I did (hips raises, prenatal yoga, rocking on hands and knees, acupuncture with moxibustion, attempted external cephalic version, etc.), nothing worked to get this girl to turn. I felt her head in nearly the same spot from 30-39 weeks gestation. Looking at the scoliosis she has, and other issues she had early on such as torticollis and slight plagiocephaly, I believe her breech presentation may have had a hand in all this.
When she was six months old, we noticed a hump in her back on her left side. She had an x-ray at around seven months, and we found out she had infantile scoliosis. It was not yet considered “progressive.” The hump we felt is actually where the rib cage slightly protrudes in the back due to the curve and rotation in the spine. Her curve (Cobb angle) measured approximately 28 degrees with a rib vertebral angle difference (RVAD) of 14 degrees. Since 80-90% of infantile scoliosis cases resolve on their own, her doctor asked us to come back in four months for another x-ray so we could see if the curve was going to resolve.
When she was 11.5 months old, we went for her second x-ray. Her curve measured approximately 23 degrees with an RVAD of 12 degrees. So, all seemed to be going great. Her curve appeared to be improving. We were optimistic that we would continue to see improvements, and so we were told to come back for another x-ray in six months. We figured we would have x-rays every six months until her curve was gone.
We started physical therapy for her around this time to help with unrelated (but maybe related??) sitting up, crawling, and muscle tone. Around five months after the last x-ray, her physical therapist and I felt that Savanna’s curve may be getting worse (or at least not getting better). However, we decided to really throw everything we had at the scoliosis, in the hopes that we could present her best spine possible at her next x-ray. I started taking her to the chiropractor once a week during the last month before the x-ray, and we ALL felt that she was improving.
In November 2013, when Savanna was 17 months old, we went for her next x-ray. I wasn’t even worried about the appointment because I felt she had improved so much. After the x-ray, the doctor came in to let us know the results. He told us that her scoliosis was now progressive, and her curve was at approximately 43 degrees! Wow… I cannot explain the shock, sadness, fear, and helplessness that my husband and I felt. Maybe if I had prepared myself for this, I would not have been so blind-sided.
Her doctor recommended an MRI scan to rule out any underlying issues that may be causing the scoliosis. If the MRI was clear, then we would proceed to casting. The MRI scan wasn’t completely clear because there is a small syrinx (cyst) in her spinal cord, however, the neurosurgeon who looked at the scan said the syrinx is not a cause for concern at this time.
So, we are on to casting now. She will need to wear a series of casts over a period of one to two years. She’ll have each cast on for 8-12 weeks, and have a few days of a break before the next cast. After her curve improves to a certain point, then we will likely move to bracing for possibly a year or so.
January 17, 2014 – Casting Day #1. We are going to Shriners Hospital for Children in Greenville, South Carolina, and we LOVE it there already!
After the first cast was applied, the doctor said that Savanna did great. She did so much better than he had expected too! He took an x-ray after he got her in the cast, and guess what?? Her curve appeared to be nearly straight! I asked him to ballpark a curve number at this point, and he said he would guess UNDER 7!!!! That is amazing to get that kind of correction in a first cast!! I knew her spine was more flexible than she was showing while she was awake! Mama knows! Now, this correction is not permanent at this point of course, but it is a great start and bodes really well for the future. 🙂 Update August 2014 – When we took her cast off on Aug. 19, it had been 9.5 weeks since she got the cast on! That was a looooooong time to have it on (especially in the hot summer), but I’m happy to report that her skin looked really good with just some minor heat rash and really dry skin, like usual. Thankfully, there was nothing worse. Needless to say, we made the most of her 5 cast-free days!
On April 19, 2006 my husband and I went in for our routine 20 week ultrasound. Long story short and many tears later, we were told our daughter would be born with an Omphalocele, basically a hernia at the umbilical cord. A few days later we had an amniocentesis performed. Ten days later, I received the call that Grace had no detectable genetic abnormalities.
Fast-forward to September 6, 2006. The day our precious daughter was to be delivered via scheduled c-section due to the predicted size of the Omphalocele. They assumed it would be large to giant in size, so at least the size of a large grapefruit. Grace was born at around 10:40 a.m. with no visible complications other than the Omphalocele. She was
rushed to the NICU where they placed a tube down her throat to suction out anything she had in her stomach. She weighed in at 8 lbs 4 oz and was 20 1/8” long. She was a BIG baby for the NICU.
Her surgeon came to visit that evening and take a look at her abdomen. Upon examination, he realized she had a considerable amount of excess skin surrounding the Omphalocele. He came and discussed with us the awesome news that he would be able to close her abdomen the following day. It appeared to him that the Omphalocele only contained part of her liver and maybe her gal bladder or appendix and with the addition of some Alloderm to allow him to close her muscles, he believed he would be able to fit everything back inside.
The next day, prior to her surgery she was x-rayed from head to toe, as well as numerous other tests, so that the surgical team could know as much about Grace’s anatomy as they could before going in.
Following the surgery, her surgeon returned to my room to let us know that the surgery was a success. While there, he asked if anyone had told us that Grace had an extra vertebra and a few extra ribs. We were very surprised as no one had told us that. He said it was probably nothing, that a lot of adults walking around have extra of both and never even know it. However, once we were released from the hospital, we would have a referral to the pediatric orthopedic clinic for follow-up.
Grace made an awesome recovery and surprised everyone when she was discharged at only 9 days old. It was estimated that she’d be in the hospital for 3-4 months.
At 6 weeks old, we went to our first orthopedic appointment. Grace’s spine was fully x-rayed. When the orthopedist came in, he showed us the x-ray. It was pretty obvious that Grace had something wrong with her back. He pointed out the very small partial vertebra in the thoracic area of her spine as well as an extra full vertebra in her lumbar region. He could find no evidence of extra ribs. The curve in Grace’s spine at the point of the hemi-vertebra was measured at approximately 23 degrees. He explained that worse case scenario the hemi would grow and Grace would have to have a fusion surgery at around 5 years of age. Best case scenario, the hemi wouldn’t grow. We were officially in the “wait and see” phase. He sent us on our way with an order to return for a new set of x-rays in 3-4 months.
This went on for about the next 18 months. We noticed Grace was having a bit of an issue climbing up on chairs. She would mainly pull herself up using her arms and once she was mostly up, she would then pull her legs up behind her. She didn’t really use her legs in climbing. Her doctor was under the impression that it may just be “her” way of doing things, but decided to have her get an MRI to rule-out any other spine/spinal cord problems. At this point, Grace’s curve measured just above 40 degrees and no other abnormalities were noted about her spine.
Over the course of 18 months, every time we were seen by the orthopedist, he would tell us that her curve hadn’t grown. His rule of thumb was that if a number measured within 5 degrees (give or take) of the last number, there was no change. So every time he measured, it was always within 5 of the previous visit, therefore, by his rules, the curve was the “same” when in actuality, her curve had almost doubled in size.
At this point I also began to notice that her lower spine was “sticking out”. When I pointed it out to her orthopedist, he said it was just muscle building up. He also continued with his stand that he would do nothing but fuse her where she was at, when the time was right.
I didn’t like that answer. I didn’t like that my daughter would have to live her entire life with a crooked spine, pain, potential respiratory issues, repeated surgeries and a deformity. At the last view of her x-rays, I could now see her spine was becoming a backwards “S”. Before the area of her spine above the hemivertebrae was straight and the lower angled out from hemi and was also straight. I searched many days on-line to find answers and came across a few scoliosis boards. It was on one of these boards that another mom recommended I get a second opinion.
A few weeks later I was discouraged when all I could find through my insurance was another doctor, who happened to be in the same clinic as our original doctor. I didn’t like the idea of basically going to the same place for another opinion and I felt they would be very biased towards the plan the other doctor had laid out.
I went back to the support board, I was beyond upset. We didn’t have the money to go outside of our insurance provider to be seen for another opinion. Again, another mom suggested that I apply to the Shriner’sHospital Network for a second opinion. I had a Shriner’s right in my own city! This I could do! I applied. It took 3 weeks to get the approval that they would see Grace and another 4 months to get in the door for our initial visit.
On July 31, 2008, we were seen for the first time at Shriner’s. It had only been about 6 weeks since she had been seen by her previous doctor and her curves were now above 50 degrees. They had grown almost 10 degrees. I nearly jumped for joy when our new doctor said he could “fix” her spine. However, Grace was still too small. So, to buy time she was fitted for a Providence Night-time Brace. She wore this brace from August 2008 until around January 2009 when she grew out of it. At this initial appointment, we were put on the surgical docket for approximately one year out (this was the typical waitlist time for her doctor).
The orthotics department measured Grace for a new night-time brace. She wore it off and on for about 2 months. She had never complained about the first brace until it was too small. However, from the first night, she complained and cried and fought us about wearing this one. I knew something wasn’t right. We went back in and saw the doctor. They did many tests with Grace in the brace and finally realized that after about 15 minutes her lower spine would rotate so much that she wasn’t aligned correctly in the brace and therefore was making her rotation worse. The braces had help hold the curves from progressing, but were basically encouraging her lower spine to twist outwards. It was so far twisted that in some positions, I could almost grab hold of her spine.
Grace was then fitted for a regular TLSO brace and was required to wear it 20 hours a day. In July 2009, our doctor said we couldn’t wait any longer, we had to schedule surgery.
On September 2, 2009, Grace was admitted to Shriner’s Hospital for her hemi-vertebra to be removed and vertebra’s T8 and T9 were fused together using hardware. She was in surgery for 8 long hours. She endured a collapsed lung, requiring a chest tube, she was placed on a ventilator, a foley catheter and had a blood transfusion as she lost a tremendous amount of blood. They transferred her to the adjacent children’s hospital’s pediatric intensive care unit. It was very hard to see her at first. She was swollen beyond recognition. She didn’t look like my sweet little girl in any way. On top of it, she couldn’t talk or move without silently crying. I would never wish anyone to have to see their baby in that condition.
The PICU nurses administered a medication to help the swelling go down. By the next morning, she was able to have the ventilator removed and at 24 hours post-op, she was returned to Shriner’s for the remainder of her hospital recovery.
The first two days of her recovery she had a plaster splint we referred to as her tortoise shell, attached to her with a very wide ace-like bandage. On the second day, she received her brace. The fourth day was her 3rd birthday and was spoiled by family, friends and of course every shift of staff at the hospital. This was the first day we finally moved her out of bed. First on pillows in a wagon, we pulled her to the playroom. Once she saw all the toys, she was much more willing to consider moving around. On day five, late in the afternoon, she finally urinated on her own and we were allowed to take her home.
One week post-op, we returned to the clinic. Grace’s curves were down to around 40 degrees. Best case scenario had always been that the curves would just go away with surgery. We discussed the options and the only one that made sense was to begin serial EDF (elongation, derotation, flexion) casting to reduce her curves.
April 2010, she received cast number 4. Her curves are down below 10 degrees in cast and with T8 and T9 fused at 5 degrees (they were unable to make it zero because it caused mobility problems), this is Grace’s “best case scenario”.
May 25, 2010, Grace moved back to a TLSO brace for the summer. This was our first opportunity to know her numbers out of cast. She is still in the mid-20’s, but that is still an improvement from the mid-40’s she was 7 months prior.
We decided to give serial EDF casting a break because Grace is also experiencing some bladder issues. In August 2010, Grace had a urodynamic test that showed her bladder isn’t emptying completely, is large in size for her age, and it doesn’t contract. I believe they are referring to it as a “Neurogenic Bladder of Unknown Cause”. We thought it was possibly due to an undiagnosed tethered cord, but a repeat MRI in September 2010 showed no anomalies other than her scoliosis that would cause her bladder to not work properly.
At this time, Grace is 4 years old. She has never been able to void on the toilet, nor have a bowel movement on the toilet. We are awaiting appointments for other opinions of her bladder problem, but as it stands, we will begin catheterizing her in the near future. This isn’t something we want to do, but in the long-term, hopefully it will avoid other bladder issues.
Our daughter, Charlee, was a healthy, happy baby. She met all her milestones and was very smart for her age. Everyone who has ever met Charlee loves her funny, happy and loving personality. We never noticed anything out of the ordinary when it came to her back. When Charlee was 11 months old she got sick (on a weekend, of course, so her pediatrician wasn’t open) so we took her in to an Urgent Care. She had caught RSV, a common illness amongst babies. The doctor suggested we do a chest x-ray to rule out the possibility of pneumonia. While the X-ray taken at the time did not show any sign of pneumonia, it did, however, show a significant curvature in her spine. We had no idea she had a curve until that point. Then we started to notice a shoulder droop, small rib hump and the curve itself. Our family still says that RSV and pneumonia save our daughters life.It is crazy the way things work out in life.
We scheduled an appointment with her doctor the next day, whom got us in contact with a pediatric specialist for Idiopathic Infantile Scoliosis. She was placed her first cast and had an MRI to rule out any cord tethering in May of 2012. At this point, her curve was 38 degrees. I left the first casting feeling very discouraged and unsure. I specifically remember being extremely emotional. I felt like was completely alone in this journey. I felt like we were not getting the answers we deserved to have as parents.
During the duration of her first cast we did a lot of research about Idiopathic Infantile Scoliosis. I came into contact with the ISOP, which was the best thing I could have done. There was so much wonderful information on the site. I felt like I was on a common ground with the other members, but mostly I felt supported and understood. None of my friends with children could relate to this situation, so it was refreshing to talk with other members that can help listen and support each other. A few other members of the group shared their wonderful stories about their experiences with Shriners Hospital for Children in Salt Lake City. Another member of the group even helped me get in contact with Shriners Hospital, so when our acceptance letter came in the mail I was more than elated!
During our first visit at Shriners Hospital they did laying and standing x-ray. This showed that she had a 38 degree curve, indicating that the first cast had produced no improvement. Disappointment began to set in for us, however we looked on the bright side and placed all our trust into DrD’Astous and his medical team. Our trust was completely valid, as they were able to correct her spine to 22 degrees with the second cast (first cast placed by DrD’Astous). The emotions of such great news were overwhelming. Each cast that was placed at Shriners improved her spine a great deal.
Charlee was seen at Shriners for the duration of 5 casts, or a full year of casting. Each cast was placed for about 2 months before it was replaced. Each casting brought a large array of emotions to our family. Adjusting to casting was a very difficult thing to do for our family. I felt very sad for us at first. I remember crying, a lot. I missed touching my baby’s back. We missed the pool, the bathtub, sprinklers in the summer and snow play in the winter, but it was completely worth it! We developed a family routine that worked for us during bath time that consisted of a lot of plastic wrap and the kitchen sink. I found great strength in the stories of other parents whom have experienced Infantile Scoliosis. Their success gave me the courage I needed during the hard times. Without ISOP, who knows where we would have been!
Charlee has been in 2 braces that she wore for 20-23 hours of the day, and one night time brace after casting was completed. Her spine was about 12 degrees when she was placed in her first brace. We were very strict about her wearing her brace at all times, unless she was taking a bath or swimming. She ended up gaining correction in her braces and I am elated to say that Charlee’s spine is currently at zero degrees!!!!! No kidding!!! Our family is nothing short of blessed to have found such a wonderful, gentle way to straighten her spine. We are so thankful! Please feel free to ask questions! Thanks for supporting ISOP!
“The casting method uses the explosive growth experienced by infants and toddlers to gently and permanently guide the spine back into its correct position,” Dr. Min Mehta said. “The earlier the treatment begins, the more likely a cure will occur.”
The innovation of the Infantile Scoliosis Outreach Program’s Early Treatment (ET) Process is that it phenomenally enhances quality of life for infants with infantile scoliosis without the invasion of traditionally prescribed, costly and dangerous surgery. Too often, surgery proves to be insignificant in the reversal of curve progression and does not attend to the desperation and anxiety families feel when imagining the future lives of their children.
When undergoing ET, children ages birth to 2 are fitted with specialized EDF casts (Mehta Growth Guidance Casts) that accelerate the body’s natural ability to self-resolve. Aiding and training the spine to grow straight, can forge a permanent path towards healthy living and completely bypasses the need for repeated surgeries, accompanied by extreme risk and financial burdens. This innovation is a form of healthcare affordability that lowers medical supply costs, requires only one night’s stay in a hospital per treatment, and limits complications. It also prevents the need for “salvage” surgeries when rods or distraction hardware must be extracted from our children before further harm occurs or when results are subpar.
Traditional medical advice employs the “wait and watch” method, calling for observation and a brace that does nothing to contribute to curve correction. In reality, the brace is only a stalling mechanism that allows spinal curves to deteriorate into a state that may jeopardize internal organs. The growth window from birth to age 2 is One such condition, Thoracic Insufficiency Syndrome (TIS), causes permanent deformities and chronic conditions that render the chest cavity unable to expand and contract for normal lung function and growth. The eventual progression of severe infantile scoliosis compromises heart and lung functions and leads to dependence on ventilators, severe deformity and shortened life span. The ET innovation is one that allows children and families to forego complicated medical interactions and doctors and patients to move forward with solutions that not only promote natural healing, but peace of mind, as well.
The study “Growth as a corrective force in the Early Treatment of progressive infantile scoliosis,” JBJS 2005 has contributed to furthering the aim of reversing progressive scoliosis in infancy by demonstrating that far from being an adverse factor, the vigorous growth in infancy is the principal force in converting a progressive infantile scoliosis into a straight spine by early treatment. This perception of growth working as a corrective force in childhood deformities should alter the aim of the treatment of infantile scoliosis from containment to cure, and (realize) a future when many more children with progressive deformity may be restored to normal appearance and function. ~ Min Mehta, MD. FRCS
Mother’s Determination Turns The Tide in Toddler’s Scoliosis Fight
Follow the long journey of ISOP founding Mom, Heather, and daughter, Olivia, as they sought to find answers where there were few, and a scoliosis treatment that would spur hope and encouragement.
As published in the Rocky Mountain News on December 19, 2000
Clinical Training for Mehta’s Growth Guidance Casting (MGGC)
For medical professionals, ISOP facilitates hands-on MGGC clinical trainings several times a year in the U.S.and around the world.
Actual case studies provide experience in the Early Treatment protocol and the precise methodologies for cast application. Training occurs in the OR of host hospitals and involves use of a specialized EDF cast frame.
Pediatric orthopedic surgeons, pediatricians, cast technicians and post op recovery staff typically attend.
Please email heather@abilityconnectioncolorado.org/newsite/infantilescoliosis to request your invitation to attend the next event.
Dr. Mehta’s Findings (The Journal of Bone & Joint Surgery, 2005)
La pequeña Sofía Egües de 3 años sufre de escoliosis infantil progresiva.
En noviembre del 2012, a pesar de haber recibido tratamiento con un corsé durante sus primeros años de vida, la curvatura de su columna había alcanzado ya los 60 grados.
Los especialistas en su ciudad natal en Lima, Perú, afirmaron que Sofía necesitaba una cirugía correctiva para implantarle unas barras de titanio a lo largo de su columna, junto a otras cirugías de mantenimiento cada 6 meses, y finalmente una fusión temprana de columna a los 8 o 10 años de edad.
“Estaba totalmente seguro que todo esto iba a destruir el futuro, el cuerpo y probablemente el espíritu de mi hija, así que de inmediato mi familia y yo iniciamos la búsqueda de otra alternativa para evitar esta cirugía y corregir la curvatura de su columna”, nos comenta su padre Ismael Egües.
La búsqueda de nuevas soluciones para la pequeña Sofía parecía imposible. Un método llamado “Mehta casting”, un tratamiento absolutamente no invasivo, sin cirugía y delicado para el cuerpo de un niño pequeño, fue su solución. “Enviamos correos a doctores literalmente de todo el mundo”, nos comenta su padre. Médicos en Perú y Sudamérica no conocían este método, y las esperanzas de la pequeña Sofía y su familia poco a poco se agotaban.
La Dra. Noelle Larson de Mayo Clinic, uno de los varios médicos que recibió el correo de la familia Egües, revisó el caso de Sofía, y al poco tiempo les confirmó la viabilidad del tratamiento con Mehta casting en Mayo Clinic en Rochester, Minnesota, seguido por aplicaciones cada 2 o 3 meses por un periodo de un año.
El Mehta casting es un tratamiento en el cual se coloca un yeso alrededor de la columna y cuerpo del niño, sosteniendo la columna erguida mientras el niño crece sanamente. “Viajar cada 2 o 3 meses a los Estados Unidos para el tratamiento estaba fuera de nuestras posibilidades económicas”, nos comenta su padre.
Ismael Egües y su familia solicitaron ayuda a Heather Hyatt-Montoya, fundadora de la organización ISOP “Infantil Scoliosis Outreach Program” de Estados Unidos. Debido a que no existía ningún médico o institución certificada en esta técnica en Sudamérica, la organización ISOP ofreció un entrenamiento gratuito en el Cincinnati Children’s Hospital para el médico de Sofía, el Dr. Raúl Macchiavello — Jefe de la Unidad de Columna en la Clínica Hogar San Juan de Dios.
Un concierto benéfico para recaudar fondos y la gran ayuda de American Airlines, con la donación de los pasajes necesarios para el viaje de Sofía y sus padres a Mayo Clinic, hicieron posible su tratamiento. De igual manera, gracias al increíble trabajo en equipo de muchas personas, se costearon todos los gastos de viaje, estadía y traductores para que el Dr. Macchiavello recibiera su entrenamiento en el Cincinnati Children’s Hospital, experiencia que repentinamente se volvió más enriquecedora ya que el entrenamiento favorecerá no sólo al médico y a la pequeña Sofía, sino a los muchos casos que vendrán en el futuro.
La Dra. Noelle Larson, de Mayo Clinic, estuvo a cargo de facilitar el proceso para que Sofía recibiera la primera aplicación de Mehta casting en Mayo Clinic en Rochester, Minnesota. En menos de un mes, la curvatura de Sofía se había reducido 10 grados con el uso de un corsé rígido, de manera que, luego del procedimiento de Mehta casting en Mayo Clinic, la curvatura de Sofía se redujo de 50 grados a 35 grados. El cambio en las radiografías era impresionante, y los cambios en la vida de Sofía fueron también inmediatos. Sofía tenía una cojera producida por la desviación de la cadera, producto de la escoliosis, pero, tan solo luego de unas horas del procedimiento, Sofía había perdido el 70% de ésta.
Ahora tiene un mayor balance en su cuerpo, y se nota al caminar y al jugar. Conforme pasaron los días, el progreso era evidente. Sofía caminaba con mayor velocidad que antes, y en sus sesiones de terapia física los logros eran indiscutibles. Tan solo un par de días después de su retorno a casa, Sofía se paraba en puntas de pies —algo que nunca había logrado—, y un par de semanas después había bajado por primera vez en su vida una escalera completa.
El Dr. Macchiavello tiene ya su cama especial EDF Casting Frame, requerida para la aplicación del tratamiento temprano con Mehta Casting. DHL Global Forwarding Perú, American Airlines y HP hicieron posible que el equipo esté listo para continuar el tratamiento de Sofía, y se asegurará que muchos niños recibirán el tratamiento temprano con Mehta casting para la escoliosis infantil progresiva.
“Desde entonces, muchos niños de nuestro país tendrán la esperanza de crecer, desarrollarse y ser felices como todos los niños en el mundo”, nos dice su padre.
“Todo esto ha sido posible gracias al gran corazón de muchísimas personas en Perú y alrededor del mundo que se unieron a nosotros en el camino, y especialmente a Dios que así lo quiso. Pero debemos mencionar especialmente a tres personas, la Dra. Min H. Mehta por desarrollar esta técnica, a la Dra. A. Noelle Larson de Mayo Clinic, que sin su ayuda esto no se hubiera iniciado, y a Heather Hyatt-Montoya de ISOP por su gran corazón”, nos dice Ismael Egües.
Por favor lea aquí para obtener información que puede salvar la vida de su niño. (Please read here to get info that could save your child’s life) Little Sofia takes big steps with the help of Mehta castin
La pequeña Sofía Egües de 3 años sufre de escoliosis infantil progresiva. En noviembre del 2012, a pesar de haber recibido tratamiento con un corsé durante sus primeros años de vida, la curvatura de su columna había alcanzado ya los 60 grados.
Los especialistas en su ciudad natal en Lima, Perú, afirmaron que Sofía necesitaba una cirugía correctiva para implantarle unas barras de titanio a lo largo de su columna, junto a otras cirugías de mantenimiento cada 6 meses, y finalmente una fusión temprana de columna a los 8 o 10 años de edad.
——————————-
Little Sofia takes big steps with the help of Mehta casting
After Mehta casting at Mayo Clinic, 3-year-old Sofía Egües saw the curvature of her spine reduced from 60 to 35 degrees and has taken steps she was previously unable to.
Three-year-old Sofía Egües has progressive infantile scoliosis. In November 2012, despite having received treatment with a brace during her first years of life, Sofía had a spine curvature that had already reached 60 degrees.
The specialists in her hometown of Lima, Peru, said Sofía required corrective surgery, which involved implanting titanium rods along her spine, as well as maintenance surgeries every six months. Ultimately, they said, an early fusion of the spine could be performed at age 8 or 10.
“I was absolutely certain that this would destroy the future, the body and possibly the spirit of my daughter,” says Ismael Egües, Sofía’s father. “We immediately looked for another alternative to avoid the surgery to correct Sofía’s spine curvature.”
The search for alternative solutions for little Sofía at first seemed an impossible task.
A method known as “Mehta casting” — a noninvasive treatment that doesn’t require performing surgery on a delicate child’s body — was identified as the best solution. Mehta casting is a treatment whereby a cast is placed around the spine and body of the child to hold the spine straight while the child grows. But physicians in Peru and the rest of South America were unfamiliar with the procedure, and the hope of little Sofía and her family began to dim.
Not ready to give up hope, then family “sent emails to physicians all over the world,” says Ismael.
Noelle Larson, M.D., of Mayo Clinic’s Department of Orthopedics in Rochester was one of the many physicians who received the Egües family email, and she reviewed Sofía’s case. Shortly afterward, she confirmed the viability of the Mehta casting procedure, which could be done at Mayo Clinic in Rochester, Minn., with follow-ups every two or three months for one year.
Traveling to the U.S. every two or three months to receive treatment, however, was not within the family’s financial capability, Sofía’s father noted.
elp from Heather Hyatt-Montoya, founder of the Infantile Scoliosis Outreach Program, which connects families of children with scoliosis with resources and information to help them make the best choices possible in the care of their child. The lack of physicians or institutions certified to perform the procedure in South America prompted the organization to offer free training, at Cincinnati Children’s Hospital, to Dr. Raúl Macchiavello, chief of the Spine Unit at the Clínica Hogar San Juan de Dios and Sofía’s personal physician in Peru. The training would not only benefit the physician and little Sofía, but also many future patients.
Funds raised through a charity concert, along with support provided by American Airlines with the donation of two tickets for Sofía and her parents to travel to Mayo Clinic, made the treatment possible. The amazing teamwork of several people covered the cost of all travel expenses, lodging and translators to enable Dr. Macchiavello to receive training.
Dr. Larson was in charge of facilitating Sofía’s first treatment of Mehta casting at Mayo Clinic in Rochester. The use of a brace decreased Sofía’s curvature 10 degrees. After the Mehta casting procedure at Mayo, Sofía’s curvature decreased from 50 degrees to 35 degrees. The change on the X-rays was impressive, as were the changes in Sofía’s life. Sofía used to limp due to the trunk shift caused by the scoliosis, but a few hours after the procedure, the limp improved by 70 percent.
Sofía now has more balance in her body, which is evident when she walks or plays. As the days went by, her progress was clear. Sofía was walking faster than before, and her achievements during the physical therapy sessions were indisputable. After she returned home, Sofía was able to stand on the tips of her toes, which she had never been able to do. Just a couple of weeks later, she descended a set of steps by herself for the first time.
Dr. Macchiavello now has an EDF Casting Frame, a special operating room table required for the early Mehta casting treatment. DHL Global Forwarding in Perú, American Airlines and HP worked together to have the equipment ready to provide continuity to Sofía’s treatment. This also will allow more children in Peru to receive early Mehta casting treatment for progressive infantile scoliosis.
“Many children in our country can now hope to grow, develop and be as happy as any other child in the world”, says Ismael Egües.
“All this was possible thanks to the generosity of many people in Peru and other parts of the world who joined us in our journey, and especially because God wanted it to happen. There are three people that deserve to be individually mentioned, Dr. Min H. Mehta for developing the technique, Dr. A. Noelle Larson from Mayo Clinic for her pivotal help in initiating the process, and Heather Hyatt-Montoya from ISOP for her big heart,” Ismael Egües says.
My story is about two of the sweetest little boys you’ll ever meet. Cameron (8yrs.) and Dylan (5yrs.) The two brothers have many things in common, such as huge smiles that light up their whole face, an infectious laugh, and scoliosis. Although they were both casted in plaster in Dec. 04, their journeys to that point and after are quite different. I’ll begin with Cameron.
Cameron was born on Aug. 28, 1999. Although he was born at 38 weeks, I started going into labor at 34 weeks. With medication and bed rest we held off for four more weeks. As all parents do, we thought our baby was perfect (and still do!) which is probably why it took so long for us to realize that something was wrong. While visiting Grandparents in Colorado when Cameron was 21 months old, his Grandmother noticed he seemed to lean to one side while sitting in the bath tub. We flew home to Portland Oregon the next day and made an appointment with our pediatrician. One x-ray later and our whole universe seemed to close in around us. When I first saw the x-ray, I had to ask “is that his spine?!” It was literally shaped like the letter “C”. The radiologist said he was surprised that Cameron was able to walk in. I was then given the x-ray to take with me to a Pediatric Neuro-surgeon. When I got home, I took it out, called my husband and tried to describe what I was seeing. It was then that I noticed the small marks and numbers drawn in pencil on the x-ray. It said 86 degrees!!! Up until that point, I didn’t realize that spines could actually bend to that degree…
The Neuro Surgeon wanted to rule out any neurological issues, and checked for a tethered cord. After MRI’s, Cat scans, and more x-rays it was determined that neurologically he was fine, but a tethered cord could not be ruled out. She said that it was in a gray area. We had a choice to make….. Our doctor said in her opinion the best option would be to do the exploratory surgery to find out. If there was no tethered cord, well, at least we would know. If we took a chance and didn’t do it and it was tethered, my son’s spine would continue to get worse. We scheduled a surgery date. On July 13th 2001, we found out that Cameron did indeed have an extremely tight tethered cord. Our doctor said it was like taking a rubber band and pulling it as tight as you can. Normally, they’re like a relaxed rubber band.
By the very next morning (post tether release surgery) his back looked better. An x-ray revealed a 67 degree curve!! Three months later at an appointment with an orthopedic surgeon, we found out his back had settled at 53 degrees!!! We were so excited, until the doctor started talking….. He said he’d never seen that much correction with a tethered cord release, before. Davie and I told him we believed it was because of all the prayers being sent Cameron’s way. The doctor then wanted to do surgery, either growth rods or a fusion. That was it….We were offered no non surgical options for my 2 yr. old. It just didn’t feel right. Something inside me said, “No surgery!”. Luckily my husband and mother felt the same way. I told the doctor thank you, but I would rely on prayer and faith to guide me and I just knew Cameron would be ok without surgery. Then, as always, life went on.
On April 17, 2003, Dylan was born six weeks early. After a short stay in NICU he went home. While I was pregnant with Dylan I was told by Cameron’s doctors that there was only about a 1 percent chance he would get infantile scoliosis. We even had an x-ray done before he left the hospital and it showed no scoliosis. And once again life went on, until he was about nine months old and we started to notice the dreaded curve. We were now living in Castle Rock, Colorado and were referred to a well known and respected Pediatric Orthopedic Surgeon. In January, we discovered Dylan had a 24 degree curve. So much for the 1 %. We also had and x-ray done on Cameron, and his curve was progressing. It was now back up to 69 degrees. We also found out that both boys had almost identical curves. Both going to the left, which is unusual in itself, and only one vertebrae apart. I’m told it’s extremely rare for two brothers with no family history of scoliosis to have it, let alone for it to be almost identical. Not that this fact made us feel any better.
After many sleepless nights, I was resigned to the fact that there had to be something new developed in the last three years. There wasn’t. I couldn’t believe I was given the same grim options. The next few months, I can honestly say, were the darkest of my life. My days were filled with guilt (did I do something to cause this?) dread, and self pity (why MY boys?). Then something changed. I had that same feeling I had three years ago in Portland. I knew there was something else out there. I became obsessed with the internet until one day I came across an organization dedicated to infants and children with scoliosis. ISOP (Infantile Scoliosis Outreach Program) was developed by a mother who also has a child with severe scoliosis. It is there that I learned about Dr. Mehta and her corrective, Early Treatment Method that did not involve surgery. After numerous hours “talking” with other parents online, Davie and I decided it was worth a shot. Cameron’s doctor wasn’t so sure, but he did however; agree to try casting the boys. We set a date and waited. As the date got closer I found out he wasn’t going to follow the Mehta Method that we had learned about and wanted. First, the doctor didn’t plan on using an anesthetic. Second, he didn’t plan on applying the jackets himself, his orthotist would. The thought of my boys being hooked up to their medieval looking machine (his words) and pulled and stretched while awake, bothered me. How could they get a good correction if my boys were tense and fighting them? Needless to say, we canceled and the plans to go to a properly trained center were in place. A date for Dec. 13th 2004 in SLC was set. By this time Dylan’s spine was at 39 degrees.
The first week they were casted was the hardest. Initially, the boys hated them. Davie and I cried with them while wondering if we had made a huge mistake, (more guilt) but as the day went on they slowly started to adjust. The next day they were up and playing. And since then, there is nothing they can’t do. Cameron snow boards and plays soccer; he can also do a summersault in a cast!! And Dylan is right behind him. I would like to point out an unexpected benefit of the cast that we noticed right away. Cameron had been suffering for the last year from severe constipation. He was even hospitalized for it. He was in constant pain and nothing seemed to help, not diet changes or even medications. Within a few days of receiving a proper plaster cast, he was regular! And has been ever since. His doctors think his scoliosis was some how causing the constipation issues and I believe it!
With every cast they both showed improvement, sometimes in degrees, sometimes in rotation or just in the way they looked. In May of 2005 they were cast by Miss Mehta herself. It was with her cast that they showed the most improvement. After looking at Dylan’s x-rays, Miss Mehta predicted that Dylan would experience complete curve resolution. And she was right! After examining him again in the fall of 06, she said he was done. And to this day he is still holding at 8 degrees! Cameron is also doing well; he’s at 34-38 out of cast. He has gone so much farther then anyone imagined. Without growth spurts on his side, though, there is only so much correction that can be expected. I would like to give everyone the exact amount of improvement from each cast; unfortunately we lost all our records in a house fire last summer.
I would like to point out now, how different their outcomes are. It’s like looking at a “what if” picture. Since their curves are so similar you can see how critical early intervention is! If Cameron had been treated early with casting when it was first noticed that he had progressive infantile scoliosis, I believe his results would’ve been like Dylan’s. Also, if we would have done the “wait and see” with Dylan, he would not be straight now.
From experience I can tell you how much easier it is to cast a younger child, not only because you have growth on your side, but little kids tend not to be as self conscious. As Cameron gets older, the harder it gets for him. Other kids opinions matter more and kids can be cruel when someone is “different”. Dylan never realized he was considered different. It never fazed him.
Although it is too late for me to change Cameron’s past or outcome, I hope his story helps convince others of the importance of early intervention. Dylan’s situation could have been similar to Cameron’s without early treatment. Just as Cameron’s spine could have grown straight gently & permanently with Early Treatment, just like his little brother Dylan’s. I hope by telling this story we can have more “Dylans”.
At this point we are considering options for Cameron. Our goal is to keep him under 40 degrees and get as much correction as possible. I’ll post any updates as they happen. Please feel free to email me with any questions.
Cole was born on January 3rd, 2008, 1 hour before his due date, after an uncomplicated pregnancy and delivery. He received 10’s on his APGAR. The only funny thing about him was that his foot was bent up so his toes touched his calf. They reassured us that it was just because I was very tiny throughout my pregnancy and he must have been cramped. Otherwise there didn’t appear to be any problems.
Within a couple days of being home I noticed that his head was slightly misshapen and that he didn’t like to nurse on one side. His doctor reassured us that it was fine. We should keep trying to get him to nurse on the side he didn’t like. By 6 months he still did not like to turn his head to that side and the doctor kept telling me to keep trying to encourage him, and that because he could do it there was no reason to worry. Both the head shape and turning we later found out were related to his progressive infantile scoliosis.
At about 10 months, while bathing Cole, we noticed that he was developing a rib hump on the left size of his back. I brought it up to the doctor at a his 12 month check up and he didn’t think much of it. We started to notice a slight curve
in his spine, but only when he sat in certain positions. I brought it up again acouple months later at a sick visit, and mentioned that I thought it might be scoliosis, because it runs in my family. The doctor said it was too hard to check at this age, and that they wouldn’t treat him until 2 even if that is what it was. Finally by about 15 months Cole started to stumble when he walked, despite having been walking by 10 months, and started needing to hold his arm out at an odd angle to balance himself. At this point we became increasingly concerned and started to do some research. My husband found ISOP and knew immediately that Cole must have Progressive Infantile Scoliosis (PIS) after seeing the pictures of some of the other kids’ backs. We scheduled another doctor appointment immediately and went in armed with Dr. Mehta’s Growth as a Corrective Force article. Our doctor reluctantly sent us for x-rays reassuring us that as long as Cole was in a brace by his teens, we would be fine.
We got his x-rays and they came back at 45 degrees standing. We got a referral to a local orthopedic for the next week and immediately scheduled an appointment at the Golisano Children’s Hospital at Strong Memorial in Rochester to have him seen. The appointment with the local specialist didn’t go well. They wanted us to hold him in a Risser cast as long as possible then move on to growth rods until they could fuse his spine. 2 months later, when Cole was 17 months, we were seen in Rochester for Cole’s 1st cast. His curve had progressed from 45 degrees standing to 47 degrees laying down with an RVAD measured at 25. The casting went well and they got him down to 23 degrees in cast.
After his casting Cole got his MRI which revealed a small Chiari I malformation in his brain. At this point it is very small and only needs to be monitored. Otherwise, Cole is a healthy, happy and very active 2 year old, who has adapted to his cast very well. He is still the fastest and most active amongst his peers. He loves to show his cast off to everyone and makes sure to tell them how much he loves it. When he gets a cast break, he asks for it back on.
After 1 year and 5 casts Cole is now able to move into a brace. He surprised us all, when he jumped from 13 degrees down to 2 within a single cast. We now get to take him home in his new rainbow brace for a calm 6 months, of summer fun, and no doctors appointments! We couldn’t be happier with Cole’s progress and are so grateful to Dr. Mehta for her incredible work, Heather and ISOP for connecting us to this treatment which has cured our baby and to our fantastic orthopedic surgeon at Strong for getting us to where we are today! We can’t even imagine where our life would be today without the combined help of these 3 different people.
Alexandra (Aly) was born in May 2010 by c-section after a normal pregnancy. She was big, healthy and beautiful!
Around 10 months old, while bathing her, her dad and I noticed that she sat a bit crooked. We brought it up to her pediatrician, but he told us not to panic. Because she was such a big, chubby girl, he believed that she was just learning to hold herself up.
At one year, it hadn’t changed, she was now walking, and we noticed a curve of her ribs on one side while bathing her. At her 12m check up, the pediatrician looked a little deeper, and set us for a spinal x-ray. He got back to us within 24 hours and said that the local orthopedic surgeon had set us up an appointment at Shriner’s in Philadelphia. The thoracic region of her spine measured an approximately 60 degree curve.
When meeting with the doctor at Shriner’s, it was decided that Aly would undergo a series of casts to gently correct her spinal curve.
The first cast was the hardest, for sure! New territory for parents, and baby. Aly had just recently learned to walk- and now having the cast down around her hips, it had to be relearned. Adjustments were made for maximum comfort at all times. Bathing and diapering presented challenges, but we had wonderful support from other ISOP parents who had great tips!
Two and a half years, several casts, and 3 custom braces later, Aly’s curve seems to be holding at 17 degrees (thoracic) and 14 degrees (lower). What used to be day to day challenges with bathing and motor skills are now every day parts of life! We are so grateful to her doctors, nurses, and our ISOP “family”.
At the May meeting of ISOP’s Physician Advisory Board, the Board resolved several key elements to successful Mehta Growth Guidance Casting:
Agreed: Underarm Casts are only effective for curves T8 and lower. Overarm Casts address all curve types.
Agreed: Modifications and/or decorations to casts, as well as cast removal at home should all be discussed with the treating physician prior to any changes being made.
The topic of cast decoration recently surfaced on the Early Onset Scoliosis & Mehta Casting facebook page:
Avery was born on October 8th 2009, weighing 3lbs 2oz. She and her twin sister Addison were 10 weeks early. Avery was my eager one and is the one that decided to come early. They had to force Addison to come out.
Avery would spend 7 weeks in the NICU 60 minutes away from home. The hospital where I delivered did not have a level 3 NICU. At her lowest, Avery was down to 2lbs 15oz. She came home at 5lbs 6oz.
From the beginning Avery has been the one that has always kept us on our toes. She had reflux from the beginning and was on Pepcid. I got used to being puked on from the beginning and boy was it bad. In order to keep her food down and keep her comfortable, she slept in a cradle swing or a vibrating seat. I know now that this could cause issues, but it didn’t in my other daughter, so it wasn’t the root cause of our issues. By 5 months Avery was upgraded to a stronger antacid for her tummy and was doing better.
Due to them being preemies, the hospital suggested a “First Steps Evaluation” at 3 months old (2 weeks old at adjusted age). At the evaluation, she was right on track and they didn’t suspect anything, but wanted to do a follow up 6 weeks later.
That is when it started. At her next evaluation, they noticed that she kept her head titled to one side. She was diagnosed with torticollis. I was given orders for physical therapy as well as home exercises for her neck. I kept noticing that her back was crooked, but everyone assumed this was her adjusting due to her torticollis. Her head became slightly misshapen and we had to see a craniofacial specialist, to look at the possibility of a helmet. This was due to her scoliosis.
She never crawled. But she would do her army crawl and when she would play, she would do what looked like an adorable pose on her side. It was her way of adjusting to her neck and back. We had even started putting a book under her left butt cheek to make her sit up straight in her highchair. That didn’t last long.
We went through 8 months of physical therapy and exercises, but her neck wasn’t getting better and she wasn’t crawling. We were now doing 1 day of physical therapy at our house and then traveling to a therapist 1 day a week. I even had someone suggest cutting the muscles in her neck. We finally had a different physical therapist that suggested we see a specialist for her back.
Avery was 12 months old when our pediatrician referred us to Riley’s hospital in Indianapolis. We had to wait 3 months to get in to see the specialist. This turned out to be the best thing that ever happened to us. We were one of the first patients to see the new specialist. He had just moved here from California and worked with Mehta casting there. The previous specialist did not do casting and we probably would have been given the “wait and see” path.
The first thing he did was shake his head at the idea of cutting her neck muscles and said we were doing everything right with her neck. He then ordered x-rays of her back. She came back with 39 degree curve and 20 degree rotation. Our Dr. made no promises to us, but recommended Mehta casting. He said we were a moderate case and that it should work, but no promises. He also gave us a support website that could offer more explanation and support on casting and that is how I found Heather and ISOP.
We left the hospital with orders for an MRI and a casting date for 2 weeks later.
My Uncle and Aunt went with me and Avery for her MRI. She was 16 months old at this time (13 months adjusted) and weighed 20lbs. She was sedated for the MRI and I was very nervous. I am a pretty strong person and kept it together, but I will never forget the feeling of seeing them take her back.
The MRI came back without any abnormalities, so we were diagnosed with “Idiopathic progressive infantile scoliosis”
The next 2 weeks went by very quickly. January 2011 is when we had our first cast applied. I had not had time to check out the website that was given to me, so I didn’t really know what to expect. Seeing my little sweetheart barely walking (she had just started at 15 months) in a tiny hospital gown, about did me in. She was so brave and didn’t even cry when they took her back.
I went to the waiting area in tears, but walked by a few other mothers sobbing and felt blessed. They had larger groups with them and had their children there for more serious surgeries. One woman my age was even laying on the floor with her head in her mother’s lap, just sobbing. Every time I walk into a children’s hospital, I am reminded of how bad it could be. I know now that scoliosis is nothing to laugh at, but we were in God’s hands and I just knew we were going to be okay.
That wasn’t how I felt when we got home that evening….. Avery came out of surgery fine and she was down to 20 degree curve in cast and 0 rotation. She would wear this cast for 12 weeks. However; she couldn’t sit up, couldn’t walk and couldn’t roll over. My husband and mother-in-law were at the house and they were in tears. Avery just sobbed, because she had lost her independence. My husband ordered me to take her back and have it removed. I stayed strong and found some pictures of scoliosis surgery incisions to show him that we made the right decision. I also logged on to this support website for the first time. Boy did I need reassurance. That was the worst night we have ever experienced.
Avery slept between my husband and I on a pillow for 2 weeks, until she was able to roll over on her own again. It took just about 2 weeks for her to re-learn everything and then watch out J. She is still my little trooper. I grew to be amazed at how strong she became physically and mentally. She has some of the strongest legs I have ever seen. She could go from sitting to standing without holding on to anything or touching the floor with her hands.
Within 3 months of being in cast, her torticollis had resolved itself. Simply amazing!
Casting also gave us other trials. No baths in the bath tub. Very hard to explain when her twin sister was in the bath tub. No swimming. Avery didn’t swim until she was 3 years old, but neither did her sister. We had a few ignorant people to deal with, but for the most part a lot of understanding. She once wasn’t allowed on a carnival ride, even though I explained what her cast was. So, I simply put her shirt back on and got her on the ride. No playing outside on hot days.
All of these sacrifices were totally worth it. They can enjoy these things when they are a little older, but we only have a small window to cure their scoliosis.
Avery also gained 2 inches in height in cast. The cast weighed approximately 3lbs. She is still 2-3 inches taller than her twin sister.
Avery would go through a total of 5 casts. We got down to 10 degrees in the last 2 casts, this was without the cast on, so the Dr. decided to brace.
Avery’s brace was molded from her last cast and she wore this for 3 months, 23 hours a day. At her 3 month check up, she was still holding in her brace, so we were told to come back in 6 months. We actually gained correction in that 6 months, 9 degree curve and 0 rotation, so we have now been brace free and cast free for 6 months. We go back on June 2014 for our next check up.
Avery is a super sweet and smart little girl. She is so strong and faces everyone with courage. She is my talker and confident one. She is also pretty comfortable around strangers, since she has been around so many. She takes things very personal and is a perfectionist, even at age 4. She is hard on herself and cannot stand to be wrong, or to do wrong.
What I have learned through this whole process is to trust your instincts as a parent. There are many people that I have met that have made comments such as “my daughter has scoliosis that they caught in gym and she is fine” Or, “I hate that she has to wear that cast, isn’t there anything else that you can do?”. I had a lot of support and also a lot of people that I felt did not understand my decisions.
The casing process is so new that people want to assume that you aren’t doing what is best.
I can speak from experience that casting works. I am so very lucky that Avery was under the age of 2 when we finally met with our specialist. Her adjusted age made it even better since she was really only 13 months at the time of casting.
When we walk by a stranger in the grocery store or in public, Camden will be the first to try to talk to a stranger or someone will lay their eyes on him and fall in love. He has such an outgoing personality but no one would ever know the things that that “sweet face” or “very happy boy” has been throughout his journey with Progressive Infantile Scoliosis.
Camden was born on September 5, 2012. He weighed 9 pounds exactly and he was perfect. He was a big baby for such a small mommy, which we weren’t expecting at ALL. In December of 2012 my Grandma brought to my attention that Camden’s spine felt curved, and he would lean to his right. His ribs were also protruding on one side. I didn’t think much of it because every mom thinks her child is perfect. At Camden’s 4-month check-up we mentioned something to his pediatrician; she took a look at him and ordered an x-ray immediately. We took him the next day to have the X-ray at Children’s Healthcare of Atlanta. I asked to see the X-ray after it was taken and I knew soon after looking at it, something was wrong with my “perfect” child.
Camden’s pediatrician confirmed my worst fear, he had scoliosis and his curve was 31 degrees. She referred us to a local Pediatric Orthopedic Surgeon to examine Camden and review the X-Ray. The following week we visited the Pediatric Orthopedic Surgeon where I just wanted closure to this; I didn’t want him to tell me anything was wrong. As they took us back I noticed there weren’t many people in the office, I can’t describe it…it was just eerie. The doctor came in and had already reviewed the X-ray. He examined Camden, and told us that Camden had a 23 degree angle and that he believed it was his posture. He thought that Camden would grow out of it, to do a few stretches with him a few times a day and to come back in 3 months to see if it had gotten any worse. If it had indeed gotten any worse they would have to put him in a brace so he could grow straight for a few months. So I, a young mom who again thought nothing was wrong with my child and all of the people around me were crazy for saying this… believed him. I was so happy to go home with decent news and that he wouldn’t have to have surgery or anything of that magnitude. My mom did not believe him and insisted he was wrong. I told her to stop being negative, but she was adamant.
All I have to say is, Thank God for my mom! I honestly don’t know where Camden would be in this without her. She had already done some research prior to the appointment and found Heather Hyatt Montoya and Shriner’s Children’s Hospital in Greenville South Carolina. We scheduled an appointment with a Pediatric Orthopedic Surgeon at Shriner’s for a second opinion and I was not looking forward to it, at all. I read the stories on infantilescoliosis.org and they sounded so much like Camden. I didn’t want to face the reality that something could be wrong.
The Pediatric Orthopedic Surgeon at Shriner’s read the X-ray. He said Camden’s curve was 33 degrees with an RVAD of 35 and wanted another X-ray in 6 weeks to confirm or deny that the curve was “Progressive”. He stated that with an RVAD of 35, it was most likely “Progressive” as per Dr. Min Mehta’s study.
The MRI was completed before the next X-ray at Shriner’s and nothing was abnormal (no underlying cause for the scoliosis) with Camden’s spine! Great news!
The longest 6 weeks of my life passed, and we were ready to visit Shriner’s again. His curve had progressed to a 44 degree angle, 11 degrees in 6 weeks! I was shocked! He indeed had Progressive Infantile Scoliosis. Camden was placed in a Mehta cast a few weeks later, on April 11, 2013. Camden was only 7 months old, at that time he the youngest infant his Pediatric Orthopedic Surgeon had ever casted. It was so hard to watch my baby go through that, but the alternative (surgery, traction etc.) would have been much worse.
Camden was casted every 8-10 weeks with no break. At Camden’s 7th casting appointment his doctor examined him and said he was ordering an X-ray to be done at his next preop. Keep in mind, his Pediatric Orthopedic Surgeon will NOT X-ray unless he sees no visible signs of the scoliosis due to the overexposure of radiation to such a little body. This was HUGE!!!
On July 2, 2014 Camden had a standing X-ray out of cast. HIS SPINE WAS STRAIGHT! The following day he was placed in his 8th cast for 4 weeks then he will be molded for a removable brace that he will wear 22 out of 24 hours per day to maintain his straight spine. We can see light at the end of the tunnel; our journey was nearing an end.
At Camden’s checkup with his Pediatrician, we ask how many cases of Progressive Infantile Scoliosis they have seen. The response was “None, he is the first one we’ve seen in our practice. We’ve seen it in older children, but never a baby”.
At one Camden’s preop visits with his Pediatric Orthopedic Surgeon, a statement was made that struck me….A baby grows half their height by the time they are two, it takes another 15 (+/-) years to grow the other half. If a baby has Progressive Infantile Scoliosis, the most crucial time would likely be in the first two years of life, during the fastest growing stage.
Awareness, education and early detection are key to saving our baby’s spines.
Breann was born in 1997. She was approximately five weeks premature and weighed 2420 g length 49 cm, head Her Apgar scores were 8. She was noted to cry spontaneously but her color remained dusky and she was given blow-by oxygen followed by mask CPAP because of diminished breath sounds. Following these interventions she improved in color. Because of her prematurity, ongoing oxygen requirement, and apnea she was taken to the newborn intensive care unit and placed in an oxygen-concentrating hood. Her initial exam showed the spine as being straight and no defects in the sacral area. But it was noted that she had a right hip click. No evidence of scoliosis was diagnosed until she was three months old.
She started out as a fighter and continues to do so. Her mother was her strongest advocate from the time she gave birth to Breann until she died in an accident on October 28, 2001. As Breann’s grandmother, I have vowed to continue her mother’s battle to help Breann through this ordeal of infantile scoliosis along with the support of our family.
Other problems soon arose for Breann. On January 20, 1997, it was noted that Breann had a small 1 cm hemangioma on her left upper arm. On March 3, Breann’s hemangioma was larger and she was diagnosed with probable fifth’s disease with resultant eczema. The hemangioma was surgically removed at three months. Breann was also x-rayed because of a persistent cough. Levoscoliosis of the thoracic and lumbar spine were found. Her curve was at 40 degrees by this time.
In May, at the age of four months, Breann showed evidence of head malformations. One side of her head appeared to be growing more than the other and one ear was larger. After a local doctor in Grand Junction examined her and could not identify the cause of the abnormalities (he at first suspected down’s or another syndrome), Joyce took Breann to Denver. She was examined at Columbia Presbyterian/St. Luke Medical Center and was found to have no syndromes. However, her curvature had increased to 45 degrees. Her neck lacked about 25 degrees of full rotation at four months and stretching exercises were prescribed for her. Breann’s mother worked diligently with the stretches several times a day and within a few months Breann’s range of motion had improved.
In August, at age of seven months her curvature had increased to 53 degrees. She was not yet able to sit up unassisted.
In November, at age ten months her curve was from T7 to L2 at 55 degrees. Her rib symmetry was also more apparent now. No cast or brace was yet recommended by the doctors. Breann’s mother was insistent that something be done. She continued to stay in contact with the doctor in Denver, but didn’t get immediate results. She also was spending time researching this condition, searching for methods to help Breann.
Finally after pressing the issue in February at the age of 13 months Breann entered the hospital in Denver and was placed in a Risser cast. Under anesthesia, pressure was applied to her spine and x-rays showed the curvature was pushed down to 32 degrees with the applied cast.
In March at age 14 months her second cast was applied. Her curve had gone back up to 45 degrees and with the cast was pushed back down to 30 degrees. Every time a new cast was applied, Breann had to under go anesthesia.
In April, (15 months) Breann was fitted in a TLSO brace in place of a cast. Joyce was exited about this because Breann could now have a bath! The brace was designed to come off for only a short period of time a day (about one hour). However, this brace did not work well. The Velcro straps wouldn’t hold and Breann had a hard time tolerating it.
She was place in yet another cast, which brought her curve back down to 30 degrees. In July, because of growth, her cast of only one month was removed and she was placed in yet another cast. Two months later, she once again had outgrown her cast and a new one was applied at Presbyterian/St. Luke’s in Denver. At this time, her curve was at 45 degrees in a cast and it was pushed back down to the low 30’s in the new cast. In October, only four weeks later, she was taken to Denver for another cast change because of growth. Her x-ray showed her curve at 48 degrees when she entered and it was pushed down to 28 degrees with the new cast. The doctors began to give Breann a week off between casts because of some rash and skin sores.
In November 1998, Breann was taken to Denver to have another Risser cast applied. After being out of a cast for only one week, her curve was now at 67 degrees, the highest it has ever been. This continued again in January 1999 (going in her curve was at 48 and after the new cast was applied it was down to 32 degrees.)
The casting helped maintain the curve and keep it from escalating. Her curve remained between 55 and 65 degrees which was a very large curve for such a small child.
Joyce continued to take Breann to Denver to have Risser casts applied and repaired frequently, throughout the year 2000.
In the summer of 2000, Breann’s mother and I flew to Shriners Hospital in Salt Lake City, Utah, so see the French doctor, Dr. Dubousset. We were hoping that a date for surgery could be set. However, after meeting with him and with Dr. D’Astous, we were told that Breann would have to wait for any surgery. She needed time for her lungs to mature and for her to grow as well. The recommendation was for Breann to be in the hospital for a few months, with what at first seemed to be a barbaric procedure. Joyce and I were stunned at the slides shown to us by the French doctor. A halo with eight screws was to be attached to Breann’s head with weights being added at intervals, to stretch her spine and lessen the curve. She was also to be placed in a turn buckle cast. We knew that this alternative was necessary and we trusted Dr. D’Astous’ recommendation as well. So, on October 2, 2000, at the age of 3 ½, Breann was admitted to Shriners Hospital where she remained until mid-January, 2001. She spent all the holidays there (Halloween, Thanksgiving, Christmas, New Year’s and her birthday!). Her mother remained by her bedside all this time, sacrificing all she had to help her baby. Joyce had to leave her other two children at home with family, and only took short breaks to come home to visit them when either myself or her mother could come and be with Breann. Joyce devoted her life to Breann.
When Breann left the hospital she was fitted for a brace with neck support that was designed in France and has maintained a curve around 45 degrees. It was a wise decision to have Breann be a part of this procedure, and we are hoping it is buying her the time she needs. We are very grateful for the care we continue to receive from Shriners Hospital and Dr. D’Astous.
Breann has a daily routine of treatments and exercises she follows that is a part of her progress. She does daily breathing exercises with a Bi-pap machine four times a day for 15-20 minutes, uses an inversion table 2-3 times a day, temporal mandibular disorder preventive exercises several times a day, swim therapy, cranial sacral therapy, massage, warm water treatments, etc. We are determined to strengthen and maintain her health. She is an incredible child.
Sincerely,
Lillian Blackman
Breann’s Grandmother
October 2003 Update
Breann has been in her current brace for 2 ½ years. In July, 2003, a visit to Shriner’s Hospital in Salt Lake City showed that her curve was approximately at a 57 degree curve. She is maintaining her curvature and it has not gotten worse since she was fitted with this brace. She continues to grow at a normal rate, and now weighs 50 pounds and is 4 foot ½ inches tall. She is now six years old, and will turn 7 in January 2004.
Part of Breann’s success is due to her continued therapy and exercises that we are consistent in maintaining. Breann has swim therapy every week at a local hospital to strengthen her muscles, increase lung capacity and improve flexibility.
Breann was staffed with an IEP at her elementary school where she is a first grader. Part of the IEP includes a teacher working with her daily, assisting her in the classroom and in stretching exercises. For about 30 minutes a day, the teacher has Breann hang and stretch from a bar to stretch her back, practice yoga stretches, and continues with neck and jaw exercise. This routine has increased Breann’s mobility and flexibility, as well has her thoracic rotation.
Along with the daily stretches and exercises, Breann uses a bi-pap breathing machine four times a day for about 20 minutes at each session. Her lung capacity and endurance continue to increase. She is an active child that enjoys and participates in most physical activities appropriate for her age. Even though she wears her brace for 23 out of a 24 hour day, this does not hinder her from riding a bike, running, and playing.
Breann has asthma and allergies that we continue to treat her for. She is highly allergic to smoke, cat dander, and some plants, as well as perfumes. She often gets respiratory illnesses accompanied by high fevers due to her weakened immune system. When she is exposed to any of the above allergens, it often results in a severe cough and allergic reaction that keeps her ill for days. She uses inhalers and a nebulizer often to overcome these reactions. Our hope is that she will outgrow these allergies.
Since Breann is growing at a normal rate, Dr. D’Astous expects she will need to be fitted for a new brace within the next few months. Our hope is that she will continue to be successful with a brace so that surgery can be prolonged until she is older.
Everyone thinks that their baby is beautiful and perfect from the first time they gaze into their eyes, and we were no exception. Hunter was born on September 7, 2012, via emergency c-section. High blood pressure on my behalf, coupled with him experiencing stress during contractions, led the doctor to make that decision. Though the cord was wrapped around his neck prior to delivery, our handsome little man was alert and wide-eyed as his daddy introduced him to the world weighing in at 5 lbs. 11 oz. He was 5 lbs. 4 oz. when we brought him home and throughout most of his first year, he struggled to gain weight. Hunter had reflux and colic beginning a few weeks after we brought him home from the hospital. The colic passed at about 4 ½ months and we hoped that it would be smooth sailing after that.
Hunter quickly developed his own unique personality and people continue to be enamored with his charismatic smile and contagious laugh. He met all of his developmental milestones at appropriate times, but despised being on his tummy until he was able to crawl. He always tilted his head to the right, which looked cute in pictures, but unbeknownst to us, was a warning sign.
As a sports enthusiast and former coach, my husband and I often find ourselves blissfully engrossed in the lore and competitive nature of an athletic flick. There is generally a challenge that unfolds within the film, a few details that pull at your heartstrings, and a triumphantly motivational ending. Regardless of our love of sports, that type of storyline embodies how I’ve always felt our life story should unfold.
The premise of “Trouble with the Curve”, just as is the baseball movie, is to be able to deal with whatever life throws at you. As momma to our beautifully curious little boy, Hunter, we are always experiencing adventure in our little part of the world. What my husband and I didn’t know, is that we would literally experience our “Trouble with the Curve” so soon, as Hunter was recently diagnosed with progressive infantile scoliosis and a tethered spinal cord at the age of 13 months.
At about 9 months of age, I started noticing that one side of Hunter’s back looked like the musculature was built up or stronger on the right side than the left. I asked my sister, who is our resident pediatric occupational therapist, and she gave me a few things to implement and suggested that we continue to watch him and then refer to our pediatrician. At his one year appointment, our pediatrician didn’t say that anything was out of the ordinary, so I pointed the curvature out to him. He immediately asked me to take Hunter upstairs to get an x-ray. He called me later that afternoon and said that he hadn’t seen a child this young with scoliosis and referred me to an orthopedic. Then began the whirlwind. We met with an orthopedic soon thereafter, and were immediately told, without a complete examination mind you, that Hunter would never be able to play sports or do anything active. We were overwhelmed, upset, confused, frustrated, and angry to say the least. First of all, don’t decide our child’s fate without a thorough examination or even knowing his fighting personality. Never mind the fact that if you look up the word “active” in the dictionary, that I’m pretty sure his picture is next to the definition. The ortho ordered an MRI and said he wanted to sit, wait, and watch for 3 months to see how much the curve progressed. We were scheduled to reconvene at the beginning of January. I’m not an orthopedic, but I would think if you know it’s progressing, you wouldn’t wait to see how much it is progressing. That was of course, before I know what I know now. If you have a feeling in your heart and your gut, then listen.We completed the MRI about a week later, which in and of itself was a hard experience having your little undergo anesthesia for the first time. Little did I know that would be one of many times that he would undergo anesthesia. Thank God that our brother-in-lawis an anesthesiologist and was able to explain everything to me prior to and after the MRI. He has a gift for calming nerves and easing anxiety by logical explanation. So, when they walked me back in the MRI room and they explained that Hunter may act like he’s suffocating and his eyes might roll back in his head, I was able to shake my head with confidence that I understood that it would be okay. He was right, it was probably harder on this Momma that it was on our little man. The MRI revealed that his spinal cord was tethered and that he had several syrinx or cysts within the spinal cord. We were told that the syrinx were fairly common, but the tethered cord would have to be dealt with. Normally, the spinal cord hangs loose and is able to move freely with growth, but his was pulled taut. I believe that the spinal cord of most individuals extends to end between the L1/L2 vertebrae and Hunter’s extended to the L4 vertebrae, so it was pulled abnormally low. We were then referred to a neurosurgeon, whose first available appointment was about six weeks after his MRI.
Sit and wait, sit and wait. I’ve decided, waiting is for the birds! Needless to say, Mama Bear came out and frantically started researching and looking for answers. In searching, my mom and I both came across a website for the Infantile Scoliosis Outreach Program (ISOP) and I found myself engrossed in all of the personal stories on their website. I reached out and called ISOP hoping that they could help me find some answers. That was the best phone call that I have made throughout this journey. Heather Montoya, the founder of ISOP, patiently listened and solidified my fear that waiting was NOT the answer. She asked for Hunter’s information, x-rays, and a picture of our baby. She then took our info and spoke with the chief of staff at Texas Scottish Rite Hospital, because they are the best fit for this condition in the state of Texas. Shortly thereafter, Heather worked her magic and we received a call from Scottish Rite. We were told that Hunter needed to address the tethered cord issue before he could go through the admittance procedure for Scottish Rite.
This was taken at the end of October 2013 right after his first x-ray. Hunter is actually standing straight or straight for him anyway, while holding onto the coffee table. As you can see, the curve of his spine is very pronounced and has gotten much worse since then.
December 17th came, and we met with the neurosurgeon, whom we adore and would love him to be Hunter’s primary doctor. He has a wonderful bedside manner and great sense of humor. He was very matter of fact and told us that Hunter would have to have surgery sooner, rather than later, to release the tethered cord. My husband, James, jokingly said, “We’re available tomorrow”, to which we were told that the surgery would actually very likely take place before the 1st of the year, especially since there were a lot of cancellations due to sickness. We received a call two days later on December 19th that he was scheduled for surgery on December 23rd and would be in the hospital until December 25th. Sit and wait, sit and wait, sprint! We were so thankful that the neurosurgeon was proactive and was able to get him in. The surgery was stressful for Momma and Daddy, but very successful for Hunter. We stayed in the hospital from December 23rd through about noon on Christmas Day.
I kept in contact with the nurse from Scottish Rite and as soon as Hunter was released after surgery we started moving forward with the paperwork for Scottish Rite. We were accepted into the Scottish Rite program and were assigned a consultation date of February 19th. We still had our appointment with our orthopedic in Houston at the beginning of January, so James and I discussed and decided to keep the appointment to see what he had to say. I’m an educator and coach at heart and am married to an engineer, so it’s our nature to research and prepare. By this juncture, I had joined a Facebook group for parents of early onset scoliosis and Mehta casting, and was completely engrossed in every aspect of this new found road that we were traveling. James and I went to our orthopedic appointment at the beginning of January armed with knowledge and I was ready to strike. I knew in my gut that we weren’t supposed to be treated there, but felt as though I should peruse every inch to make certain we were on the right path for Hunter. I walked into the office with skepticism and left fuming. James asked if I wanted to be mad at him, but the truth is that I just wanted to be mad. Mad at the fact that, while I’m not a doctor/orthopedic, I know that our orthopedic hadn’t done his homework. It is black and white to me. You can’t profess and implement a the Mehta philosophy and not believe in it and all of its parts. As a parent to a little man that can’t yet speak for himself, I have to question and challenge, and honestly he didn’t meet the grade. In parent/coach conferences, I used to always reassure every athlete’s parents that they were their child’s greatest advocate. That sentiment has never hit home more to me than it does now. Luckily Scottish Rite was in the horizon and we are now onto bigger and better things. The lesson, advocate for your children and what you believe in. Don’t settle for what someone tells you, research and learn the answer for yourself and challenge what you feel isn’t right. Most importantly fight and listen to your heart.
In preparing for a competition or an upcoming challenge, it is imperative that you have a game plan. That game plan may change depending on the opponent or scenario, but ultimately it’s reflective of your personnel and philosophy.
With Progressive Infantile Scoliosis, the game plan is to seek treatment as soon as possible and preferably before the age of 2. With little nuggets like Hunter, they are growing at a rapid rate, and therefore the scoliosis can rapidly progress without treatment. The sooner you treat it, the better the chances of success. Without treatment, it can lead to a lifetime of problems with deformation of the ribs, reduced lung capacity, etc.
You’ve met the personnel, our little man, Hunter, with a fighting heart. Now for the philosophy to beat this condition. PIS is a treatable scenario, but as I said before, it is very time sensitive. The ortho that we met in Houston was all about “wait and see”. His philosophy was that you perform treatment as more of a holding pattern and precursor to surgery in the early teen years. I don’t know about you, but I would rather come out fighting and try to score first, rather than sit back on defense.
Through research, and information sent to me by Heather Hyatt-Montoya, I learned of the studies of Dr. Min Mehta and her method of casting little ones with infantile scoliosis. Her mindset and philosophy was that with the cast, a child can have a gentle form of correction to guide or retrain the growth of the spine. Dr. Mehta personally trained the doctors at Scottish Rite. They adhere the Mehta torso casts in succession for a period of time determined by the severity of the curve and progress of the child. Each cast stays on a child for an average of about 8 weeks. Prior to being admitted to Scottish Rite, I had already made up my mind and heart that that was where we were supposed to be. We must allow him to be treated in the best environment possible in the most least invasive way,
Our consultation appointment with Scottish Rite was February 19, 2014, the doctor and his team came in and examined Hunter, watched him walk, held him. Hunter, of course, begins flirting with the nurse and then kissing me on the cheek to see what they would do.
We asked a number of questions and the orthopedic said that he would like to have X-rays done and then move forward with casting as soon as possible. He indicated that Hunter will be in a cast for a minimum of 1 1/2 years and he removes and replaces the cast every two months in the same procedure, so he will undergo a lesser amount of anesthesia. Music to my ears!
He said that his schedule was pretty tight but was sure that they could work us in. His nurse piped up that she thought that they had an opening for Friday and that she would check and get back with us. Friday?! What a difference a doctor makes!
Hunter completed the X-ray, was then measured for a scoliosis study, and was squeezed into the schedule for Friday. Praise God for leading us to Scottish Rite and giving the doctors the understanding of the sensitivity of time!
We began preparing as best we could for Friday by buying clothes (he will have to go up a shirt size), diapers (he will have to go down a diaper size), things for the car trip home in case he gets sick, and things to occupy little man as best we can. After our appointment we went to the home of some of our friends so Hunter could rest and stretch his legs.
Prior to making the trip to Scottish Rite, Hunter had had two X-rays with his previous orthopedic. One X-ray was taken at the end of October and one was taken at the beginning of January. The first number that we were given by the initial ortho, I believe, was 37 degrees. We were told in January that the curve had increased 7 degrees from October until January. Generally curves greater than 20 degrees are observed because they likely may resolve on their own. Curves greater than 20 degrees are addressed with some form of treatment.
(Mehta casting, while the most gentle and effective cure, is not common practice for all orthopedics. Reason being, a good number of orthopedic surgeons want to do surgery or use casting/bracing as a holding pattern prior to doing surgery. Remember, difference of philosophy. )
If a curve is greater than 40 degrees, it can be decreased, but may never become completely straight, but many get close. About .1% of children with Progressive Idiopathic Infantile Scoliosis have curves greater than 40 degrees. We knew we were probably in the danger zone. The more that I have read and the more parents that I have talked with whose children have this condition, made me have the realization that Hunter’s X-rays with the first orthopedic were incorrectly done. An accurate X-ray can be done standing or lying down. The protocol is that the arms must be at the side and not pulled above the head. If the arms are above the head then spine would be lengthened and the curve would appear straighter. His arms were pulled above his head in both previous X-rays. That in and of itself makes me want to scream! Again we are on the best path now, but incompetence makes me furious. Parents, please question what your child’s doctor does or doesn’t do for their ultimate well being. You are their voice and I can’t stress that enough.
So, prior to our first X-ray at Scottish Rite, we knew that Hunter’s numbers could very likely be much greater than what we had thought they were. His doctor solidified our fears as he told us that his curve was actually 60 degrees pre-cast. However, he also brought great JOY in the same sentence as he told us that his X-ray in cast showed that with the traction and compression of the cast that his curve was 28 degrees!
Hunter is currently in the first of numerous casts to come. He is scheduled for his next cast on April 18, 2014. Children, especially our nuggets with scoli, are resilient. He has done extraordinarily well in cast and quite honestly, better than we ever anticipated. God has big plans for our little man, I am certain of that. James and I were talking with family recently and all agreed that he has the perfect personality for challenges such as those that he has, and will face. When Hunter was born, James joked about us not receiving an instruction manual before leaving the hospital. We could sure use one about now. The truth is, you have to go with the flow and try to adapt to the curves that life throws you.
Sophia Update September 28, 2010
Sophia’s spine continues to grow straight and de- rotated. We monitor with X-rays annually, unless we see something that would give us cause for concern and we would then X-ray sooner. After successful EDF/Mehta casting 2007-2008, she wore a Providence Brace 8-10 hrs a night from Aug 2008-May 2009. Then nothing- just on going PT for low muscle tone and lax ligaments and monitoring of spine until “skeletal maturity”. She just turned 4 last week and is a happy, tall, healthy, active girl thanks to ISOP and early intervention!
Original Story:
We were blessed with a beautiful baby girl on September 22, 2006. My husband and I were delighted, as was her 2 year old big brother Samuel. Sophia was a healthy, full term infant. However, despite our best efforts to protect her during cold and flu season, she kept getting pneumonia and was hospitalized for it the first time at 2 months old. She also had recurrent atelectasis, which is the collapse of part of a lung caused by a blockage of the air passages (bronchus or bronchioles) or by pressure on the lung. Hers was mild and just a small pocket of her lung would collapse. She also suffered from mild sleep apnea, severe reflux (GERD) and gastric delay emptying (food/liquid did not move through her stomach like it should and would just sit there, often coming back up when she attempted to consume her next meal hours later). She seemed to have low muscle tone (severe hypotonic we later learned). She was like a jello baby and could not sit up or even be propped up without falling over like a rag doll. When we picked her up under the arms, it was as if she might slide right through our hands. Right before her six month check up, her daycare provider discovered her scoliosis.
That started our long and winding journey to countless doctors beginning with her pediatrician, who then sent us to a neurologist. He then ordered an MRI of her brain and full spine under anesthesia which showed a very small syrinx in her lower spine (a fluid-filled cavity within the spinal cord. We were told that this is something often seen in normal individuals and does not cause scoliosis or need treatment.). We were then sent on a search for a pediatric neurosurgeon. The first neurosurgeon we consulted later pulled in his orthopedic counterpart, who by the grace of God was familiar with Dr. Mehta’s EDF (elongation, derotation, flexion) casting method and early treatment for progressive infantile scoliosis (also the first to provide an actual diagnosis for Sophia’s condition). We knew it was progressive since we had multiple chest x-rays from 2 months old to 6 months old and in hindsight could see the curve forming, plus an RVAD measurement 32 degrees. We were then faced with determining a treatment plan for her. We consulted three well respected pediatric orthopedic surgeons from around the country and received three different treatment recommendations: 1) Brace her to slow the progression 2) Cast her immediately in a traditional Risser cast since it was progressing so quickly and she was too young for spine fusion. However, he was concerned that the cast might make her pulmonary problems worse and could cause chest wall deformity. He warned us that she would face surgery in her early life and beyond. 3) Travel to Shriners Hospital in Erie, PA for Mehta casting specifically since only a few places in the US offered this treatment with the correct equipment and training.
I then dug deeper into my research on Risser vs EDF/Mehta casts for non structural progressive infantile scoliosis. After a few long nights of reading everything I could find in countless websites and medical journals, I found the ISOP site www.abilityconnectioncolorado.org/newsite/infantilescoliosis and the CAST support group. Heather and the others provided the critical information and support that allowed us to make an informed decision regarding the right treatment for our daughter. By finding out about Early Treatment when Sophia was so young, we were able to harness her rapid growth during the first two years and not just slow the progression but correct it! It also treated the rotation of the spine, which in Sophia’s case we were told was significant. This treatment has allowed her to escape a childhood filled with painful and dangerous surgeries required to save her life. Instead, we were able to gain access to a non-invasive, gentle form of correction that has “taught her spine to grow straight”.
We drove from our home in Indianapolis, IN to Shriners Hospital in Erie, PA to have Sophia’s first Mehta cast applied in June 2007 when she was 8 months old. She had a total of 8 casts done in 14 months. Sophia transitioned to a Providence Brace in August 2008, which she wears 11 hours at night only. She can be a normal, healthy child the rest of the day. Check ups with x-rays in October 2008 and March 2009 showed that her spine is staying straight and de-rotated. We will have another check up in 4-6 months and continue to brace at night until then.
Her sleep apnea has resolved, her reflux and GI problems are greatly improved and she is eating and growing like crazy (90+ percentile on height and weight now!). While her muscle tone has improved, she is still on the low side. She is prone to pulmonary issues, but went an entire year without any problems. Overall, by correcting her spine, we have greatly improved her overall health. We also saw a genetics specialist who tested for everything they could test for and found nothing. So Sophia really is one in a million!
Below are the before and after measurements of each of her 8 casts. Due to many factors, including doctors changing hospitals, the chance to be treated by Dr. Mehta herself, and finding the right treatment fit with a particular program, Sophia was treated at multiple locations across the United States. We are grateful that we now have options when just a few short years ago, there were only two locations in the US that had the training and proper equipment to provide this life saving treatment. And before that none! I can’t thank ISOP and Dr. Mehta enough for all that they have done. Their commitment and dedication to this cause truly has changed the course of Sophia’s life. We will be forever grateful!
Cast#1: June 7, 2007
COBB 36 degrees out of cast -> 29 degrees in cast
RVAD 32 degrees out of cast -> 27 degrees in cast
Significant rotation
Cast#2: August 9, 2007
COBB 36 degrees out of cast -> 25 degrees in cast
RVAD 33 degrees out of cast -> 22 degrees in cast
Significant rotation
Cast#3: October 15, 2007
COBB 22 degrees out of cast -> 17 degrees in cast
RVAD 18 degrees out of cast -> 35 degrees in cast
Cast#4: December 11, 2007
COBB 20 degrees out of cast -> 7 degrees in cast
RVAD 35 degrees out of cast
Cast#5: January 28, 2008
COBB 20 degrees out of cast -> 0 degrees in cast
RVAD 35 degrees out of cast
Cast#6: February 14, 2008
COBB 19 degrees out of cast -> 11 degrees in cast
Significant rotation
Cast#7: April 10, 2008
COBB 11 degrees out of cast -> 7 degrees in cast
Cast#8: June 3, 2008
COBB 11 degrees out of cast -> 5 degrees in cast
Minimal to no rotation
Transitioned to Brace: August 2008
COBB close to 0 degrees out of cast (too small to measure)
No rotation
Everyone who meets my son, Jackson, immediately thinks he is quite the charmer! I sincerely believe that is partially due to his innate personality, and partially due to the resilience and character he has developed on his journey with Progressive Infantile Scoliosis (PIS).
Jackson was born on May 5th, 2010, weighing a very average 7lb 6oz. He very quickly became the love of my life and a very happy baby. Other than his reflux, Jackson seemed to be healthy and thriving. When Jax was 4 months old, my husband expressed a concern to me that he thought Jackson’s back looked crooked. I didn’t think much of his comment and assured my husband it was probably because Jackson’s core muscles weren’t yet strong enough to support his weight. The very same day, my mother said to me: “Sometimes when I’m rocking Jackson to sleep, it feels like one side of his back is bulging.” Suddenly, I began to worry that something might be awry with my seemingly perfect little guy.
Being a pediatrics registered nurse myself, I felt ridiculous making that first phone call to Jackson’s pediatrician (where I worked at the time) and asking for an appointment because “Jackson’s spine looks crooked.” In retrospect, it was the most important phone call of Jackson’s life. One glance at Jax, and his doctor immediately referred us to a well-respected children’s hospital for an orthopedic consult. Although, only one week earlier, Jackson had had his 4-month well check up, and his spinal curvature had been completely overlooked. *** An Infantile Scoliosis exam is now part of routine baby well visits at Jackson’s pediatrics office! ***
As soon as we returned home from the pediatrician’s office, I went into research mode and began searching the internet for reliable literature on Infantile Scoliosis. I found very little information. What I did find, presented only “doom and gloom.” I even brought out my pediatric nursing textbook which contained exactly one sentence on the subject: “Scoliosis with an onset before age 3, having a very poor prognosis.” My head was swimming, my heart was pounding, and I felt utterly alone. That’s when I discovered the website for ISOP and soon connected with Heather on the telephone.
My discovery of ISOP was truly a turning point for me. It gave me valuable resources and the confidence to utilize them. In a matter of days, I cancelled Jackson’s appointment with the local children’s hospital and made an appointment with the Shriner’s Hospital Network. Jackson was first seen in Philly at age 5 months. There, his first x-rays were taken, revealing a COBB of 20 degrees and an RVAD of 18 degrees. Because Jackson’s measurements were truly “borderline,” we were instructed to watch and wait for 3 months. During those 3 months, Jackson had an MRI which was thankfully normal. From age 5 months to 12 months, Jackson’s curve and RVAD (rib vertebral angle degree) stayed mostly stable. We continued to “watch and wait” to determine if my son’s scoliosis was of the progressive nature, or not..
Suddenly, Jackson’s x-ray taken at 14 months old revealed a COBB for 45 degrees. His scoliosis was now clearly progressive, and it was time to take action! Jackson was scheduled for his first Mehta cast at the Shriner’s in September 2011, when he was 16 months old. That first cast was difficult on all of us – probably more so on mom and dad than on Jackson. It took our little man about 2 weeks to re-learn how to sit without support, play on the floor with his toys, and run around. Soon, however, he was back in full swing!
Jackson’s first 5 casts were applied at Shriner’s in Philadelphia. Thankfully, the combined efforts of those 5 casts corrected Jackson’s standing, out-of-cast COBB from 45+ degrees to 18 degrees. After Jackson’s 5th Mehta cast, we made the decision to transfer Jackson’s care to Shriner’s Hospital in Greenville, South Carolina. We wholeheartedly believed in Dr. Min Mehta’s EDF casting methods and the integrity of her work and wished to continue with Mehta casting to treat (and hopefully cure) Jackson’s PIS. Our family just needed to do so in another place where where Dr. Mehtas techniques were being followed to the letter. ie: Jackson was able to benefit from a cast without shoulder straps because the location of his curve was low. A curve above T-8/9 is best addressed by a Mehta cast with shoulder straps.
The Shriner’s Hospital in Greenville, SC is an incredible place! Jackson now looks forward to going for his specialized EDF Mehta Casts. Prior to Jackson’s 8th casting, his standing, out-of-cast COBB measured only 4 degrees! Jackson’s orthopedic surgeon in Greenville is strongly committed to maintaining this correction, so he has continued to cast Jackson in order to train Jackson’s muscles and ligaments to maintain this straight spinal alignment. In March 2013, Jackson had his 9thMehta cast applied. For the first time, we were instructed to return to Shriner’s Greenville WITHOUT REMOVING this 9th cast because there is a possibility it will be used to construct Jackson’s removable brace. Jackson’s doctor is aiming for a 0 degree measurement before graduating Jackson into a brace.
When we returned to Shriners on May 22, 2013, Jackson’s x-rays showed that his spine measured 0 degrees! He was completely straight! Jackson’s doctor opted not to cast Jackson a 10th time, but instead to mold him for his TLSO brace which he received in early June. We continue to be overjoyed and utterly thankful for all those who played a role in CURING our son! “Cure;” what am INCREDIBLE word!
Still, Jackson will continue to proudly lift his shirt and show the world his BRACE! He is so proud to wear his new brace and often proclaims “I love it!” to anyone who asks. It has not hindered his spirit in the slightest.
In his Mehta cast, Jackson: rode a rollercoaster, becamea big brother, took a train ride, petitioned Duck Tape Brand to donate a display to Shriner’s Greenville, hunted for Easter eggs, met The Wiggles, watched a monster truck show, played soccer and baseball, learned to use chopsticks, went trick-or-treating, traveled to DC, went to preschool, and developed wisdom well beyond his years. He is a true hero in my book!
before and after xrays Jackson’s measurements: (standing, out-of-cast)
Prior to Cast #1: COBB 45+, RVAD 30+
Prior to Cast #2: COBB 40, RVAD 26
Prior to Cast #3: no standing, out-of-cast x-rays
Prior to Cast #4: COBB 22, RVAD 22
Prior to Cast #5: no standing, out-of-cast x-rays
Prior to Cast #6: COBB 18, RVAD 4
Prior to Cast #7: no x-rays
Prior to Cast #8: COBB 4, RVAD 0
Prior to Cast #9: no x-rays
Prior to TLSO Brace: COBB 0, RVAD 0
Jennifer (Jackson’s Mom)
Pediatrics Nurse
Photographer with Favorite Things Photography
“We are the music makers, and we are the dreamers of dreams.”
– Willy Wonka
Andrew’s life started with a full term pregnancy and a healthy baby born to a couple just about to celebrate 3 years of marriage. This story your about to read is long and includes a lot of details that might not seem significant to his scoliosis journey but I think it’s important to paint as clear a picture as possible of what life was like for us and hopefully encourage you when the road feels dark and overwhelming and give you hope that you can make it through this and that it is worth it.
At 10 days old, Andrew started “spitting up”. (more like a waterfall pouring out of his mouth) Seemingly everything that went in his tummy, was coming right back out. After talking with the advice nurse, we took him to the hospital within just an hour or so of onset. The amount of spit up combined with his tiny newborn size, he was already dehydrated on arrival. He wouldn’t hold anything down so an iv was needed. After the hospital tortured my tiny little 10 day old baby trying to get a needle in, they decided to transfer us to the children’s hospital. After admitting Andrew as inpatient, running a series of blood tests, stool and urine samples, getting an iv in for 4hours before it fell out of his scalp, he kept just enough in to gain a few ounces so they sent us home saying he must be fine. The vomiting continued and we were seen outpatient for imaging and weight checks as he struggled with dangerous weight loss. After everything was ruled out, he was finally diagnosed with reflux. Andrew’s reflux was so severe that he was diagnosed as failure to thrive and was in a constant battle to get anywhere near the growth chart.
At a feeding clinic for the reflux, they did a full exam and in addition to being low tone, I was told Andrew had torticollis. I was given all kinds of suggestions and exercises to do at home to strengthen his sternocleidomastoid muscle. Nothing worked. At 6 months old, Andrew was referred to physical therapy through Early Intervention. On our very first visit, the PT asked to strip Andrew down to diaper and look at his whole body. She looked at his spine and it was very clearly curved. She explained to me that scoliosis wasn’t a life threatening situation and some people live with it for a life time. She called the pediatrician and told him her findings and Andrew and I went into see him for an appt. Andrew was sitting on my lap in a diaper with his back to the door when the doctor walked in and he saw the curve with the naked eye immediately. We were both baffled. This giant curve seemed to appear overnight. We had been in clinic several times a week for months for reflux and growth problems and had never seen a curve. It’s hard to know now if it had been obvious much longer and we just missed it focusing on other issues or if it truly progressed as rapidly as it had seemed.
The pediatrician referred us to an orthopedic specialist at our local children’s hospital where they did xrays and confirmed the scoliosis. He measured Andrew’s film at 45 degrees and told me we would need an MRI to look for any congenital abnormalities that might not show on the xray. The ortho told me there was no rush. This wasn’t anything to worry about right now and sent us on our way. Leading up to this appt, I had googled unsuccessfully night after sleepless night trying to learn something about scoliosis in infants. At one point the ortho mentioned cast and that one word is what led me to www.abilityconnectioncolorado.org/newsite/infantilescoliosis and the Yahoo support group. That one word he casually threw out is what essentially changed our lives because it got me on the right path.
I didn’t hear anything about scheduling the MRI for a few weeks, so I called and finally got it scheduled, again with no urgency except for my own. The MRI results were sent to a neurosurgeon in the same children’s hospital as our ortho. The radiologist report said there was no evidence of tethered cord. Thankfully the neurosurgeon read the films himself because Andrew did indeed have tethered cord as well as syringomyelia. We had a follow up MRI to check for chiari malformation which was negative.
The ortho wanted to just monitor Andrew without any intervention. Wait and see. My baby was struggling to survive with severe reflux causing failure to thrive, delayed gross motor skills, a tethered spinal cord and now an aggressive scoliosis that was trying to crush his heart and lungs and the doctor wanted to wait. Scary. Scary as a first time mom. Scary as any mom. Scary. Period. I didn’t know much about casting yet but I asked him if he had heard about Mehta casting because of what I had read and heard from other families on the Yahoo support group. He said he had heard of it and knew a doctor in New York that could probably talk him through it over the phone. I never went back to that doctor again. I’m sure he’s a very qualified doctor for other pediatric orthopedic conditions but it was clear progressive infantile scoliosis was not one of them.
Andrew was unable to sit unassisted or bear weight on his legs at all at this point. His motor skills were getting further and further behind and his outlook looking more and more difficult. At 11 months old, Andrew had surgery to release the tethered cord. The surgery was smooth and aside from a site infection that cleared with a round of antibiotics, there were no complications.
After researching options and talking with families that were gracious enough to share their very personal stories, I knew where I wanted to go for treatment of Andrew’s progressive infantile scoliosis. I knew what I wanted for my son but I didn’t know how to get there. I knew I needed to travel out of state to get to the hospital I could trust to treat this very complex condition. I knew I couldn’t afford it. Shortly after Andrew was born, I quickly became a single mom despite all my picture perfect plans for our family. I was doing this alone and I didn’t have money and I was exhausted and scared and had no support system behind me.
There is a hospital local to us that does casting. They call it Mehta casting. They have the proper casting table. I knew in my heart though that they weren’t doing proper Mehta casting and I knew in my mommy gut that this wasn’t the right place for us to be. I applied for that hospital because I needed a plan. I knew I didn’t have to go there but if I couldn’t get to the out of state hospital, this was the best I could do. I felt sick about it, but I had to at least do something to start. Precious time is ticking. Early treatment in vital. These words kept repeating in my head day and night. We got accepted to this hospital and I felt zero relief. I was heart sick about it.
With our appt scheduled at the local casting hospital, I finally got the courage to apply to the out of state hospital. I didn’t know how I was going to get there. I didn’t have anything figured out but I knew that’s where we needed to be. That feeling never wavered in my heart. I knew.
While waiting for paperwork to process at the out of state hospital, we had a consult with the local casting hospital. You know those situations in life where you just know something isn’t right? I felt that. I felt it deep. The doctor did not have a bedside manner that gained my trust, he was shouting to a staff member in the hallway right in our sight. I felt awful there. When I asked questions, I was treated poorly and as if I shouldn’t be asking the doctor questions. I was the mom, he was the doctor. He was the boss and I wasn’t. My heart hurt. I was scared for my son and did not feel good about this connection or trusting my tiny little person in this doctor’s care. I set the casting appt there because I had to. I couldn’t travel out of state. I couldn’t afford it. I couldn’t do it alone. My husband was gone, I needed to work.
Then the letter came from the out of state hospital accepting my son. I was over the moon. I cried tears of joy and held my baby and assured him everything was going to be okay. We were going to make it. We were going to do it. I didn’t know how but it was happening. It. Was. Happening.
The care coordinator at the out of state hospital and I had a long phone conversation discussing what was next and what to expect and she answered all my questions. I just needed to wait for a call back with a casting date and we were set.
Then she called back. She told me the doctor at the out of state hospital reviewed our case and determined our local casting hospital could handle it. I was devastated. I hung up the phone and cried my eyes out. Heart broken and scared. Again. I was in the car when I got the call and as soon as I got back home, I went straight to the yahoo group and shared what was happening. We were being stopped from going to the hospital I trusted by logistical red tape. At this point, the families on the support group were my life line. They knew. They understood.
A family on the Yahoo group who are patients at the hospital I was trying to get Andrew to heard my cry for help. They talked to the care coordinator at their next visit and explained our story and my heart for my son to be treated there. The family came back and told me they found out I could fly down to the out of state hospital for a clinic visit to meet the doctor and let him see my son in real life rather than his medical file and see if he would reconsider Andrew as a patient.
Time is ticking. Early treatment is vital. The words continued to echo.
I went ahead and kept the casting appt at our local hospital hoping that any cast would be better than no cast. We got Andrew’s first cast locally and I was so sad. The cast didn’t have plaster of paris, it didn’t have a cut out in the back for rotation, it wasn’t perched on his hips which caused it to shift around on his tiny body. I couldn’t wait for our out of state clinic visit to meet the doctor I wanted and to show him the type of cast that was available to us locally.
2 weeks after Andrew got his local cast, we were on a plane to the out of state hospital. We had a clinic visit, I shared my concerns with the doctor, he did a thorough exam of Andrew, re-measured his spine which was actually 60-65 degrees with rotation, and we left that day officially accepted as patients to the hospital I trusted and knew without a doubt was doing proper Mehta casting and had a high case load with a lot of expertise for cases just like Andrew’s. We still had a very long road ahead of us but for the first time, I felt some peace that everything just might be okay.
We flew back a month later for a casting date. Andrew woke up from anesthesia but his oxygen saturation was low. He was very worked up in recovery, so they let him come back to his inpatient room still on oxygen so he could be with mom and hopefully calm. In addition to low O2 sats, he wasn’t acting like himself. He wasn’t recovering from anesthesia like he always has at home. He started becoming weak and unresponsive. The room filled quickly with doctor, PA, anesthesiologist, nurse, charge nurse….it was suddenly all hands on deck. They took Andrew from my arms and put him on the hospital crib. Checking his cast, his vitals, everyone talking collectively and no room for mom to be near anymore. I was terrified. He was given narcan to reverse all the meds he had on board and that brought him back to baseline with the exception of oxygen. He wasn’t able to breathe room air but was responsive again and it looked like we were out of the danger zone. After much review and discussion, it was determined Andrew was not acclimating to the change in altitude from our home state to the hospital. I was heart sick. I have just fought against so many challenges to get him here and here makes him sick.
We came home and saw a pulmonologist. He diagnosed Andrew with restrictive lung disease and agreed Andrew could safely fly and be at elevation….with oxygen. A baby on oxygen just to get to an out of state hospital to get a cast that some people tell me we can get done locally? My heart knows otherwise. We powered through. I started the fight to get oxygen equipment. Insurance was refusing it and now I’ve got travel expenses and portable oxygen rental. There is no way I could afford all of this. I was told that some local shrine’s help with travel expenses but because we had a local hospital we could go to, that there is no way they would cover our expenses to get to a different one.
I tried anyway.
They accepted us. No questions asked.
I got approval to pay for our travel to the out of state hospital without an ounce of hesitation from a group of kind hearted generous men who had never even met us before.
So, 6 weeks after our first out of state cast, we were ready for the next cast trip with oxygen in tow. Let me just brag on my son for a minute. That kid is amazing. He played and laughed and giggled and could care less that he needed a canula in his nose to breathe. Kids are strong resilient little people and my son was no exception. Never ever doubt your kiddos or let your fears control their outcome. They got it handled. Totally.
After months of advocating and fighting like crazy, insurance approved the oxygen. When it comes to your kiddo’s health, fight. When you feel like giving up, fight. When it feels like you’re totally defeated. Fight more.
We travelled for a series of 8 casts, 2 full time braces and 2 night time braces. There were times of celebration and times of defeat. When we got to our 6th cast, things started to feel a little dark. We weren’t making progress and my dreams of a cure seemed farther and farther away. Guess what? Good doctors don’t quit! The PA gave me a pep talk and told me we’re going to keep going. We’ll keep going as long as we have to. We’re not giving up. The very next cast, Andrew’s spine was completely straight in cast. We went from fear to victory in ONE CAST!
We casted for 14 months, we braced full time for a year, we did night time bracing for 6 months…..Andrew looks phenomenal. His neck straightened, he learned to walk, he learned to run and his spine is completely straight. 2 ½ years ago doctors told me he would need spinal fusion in a year. 2 ½ years ago doctors said his outlook was poor. 2 ½ years ago, I am the only one that believed in a miracle. Today, we have it. Today, we are celebrating a straight spine in my son’s body. We gave up baths and sand and beach days for a while but the rest of my son’s life is saved. Absolutely none of what we had to miss matters now, not one single thing.
Metha casting works. Early treatment can be a cure. Fight for your babies mamas and daddies. It’s worth it.
We were so excited when we found out we were pregnant with our first child!
On Tuesday, October 5th, 2010, Brayden Richard was born via c-section at 11:33 am. He came out screaming and hasn’t stopped talking since.
After his 2nd appointment with the pediatrician we were off to the local children’s hospital for testing when Brayden was 10 days old. He was having troubles keeping food down and I was breastfeeding at the time. He was diagnosed with reflux. We ended up seeing a gastroenterologist and had a couple more tests run to make sure there was not anything else wrong. Everything led us back to Brayden having reflux.
Being first time parents we were worried about our son getting enough nutrients after being diagnosed with reflux. Little did we know this was just the beginning of what was yet to come.
Between the age of 3 and 4 months old, Brayden has been in the hospital with bronchiolitis twice and was also diagnosed with torticollis. We were becoming very familiar where things were located at our local hospital. Our pediatrician recommended physical therapy so that’s what we did.
At 5-month’s old, we noticed a rib hump on his chest. We asked his pediatrician about it. He said it was probably extra cartilage and to monitor it for a few weeks. If it got worse we needed to call and he would get us in for an X-ray. It was not any better and seemed to be getting worse so we went for the X-ray. Our pediatrician called with the results and we were not prepared for what we were about to hear. Honestly, can anyone ever be prepared for hearing something is wrong with your child?
We got in to see the Pediatric Orthopedic Surgeon within a couple of weeks. He confirmed the diagnosis of Progressive Infantile Scoliosis (PIS). He had convinced us that in a lot of cases, this corrects itself and to continue physical therapy and come back in 4 months and have x-rays taken again. You know…the watch and wait game? So we played it because we did not know any better and trusted our doctor. He seemed to be doing better at 10 months when x-rays were taken. He said we need to wait until Brayden is walking to get a “true” reading on the x-ray and this would give a better idea if his PIS was correcting itself or getting worse. So we continued physical therapy and played the watch and wait game again.
Brayden began to walk at 12 months old and at 14-months old, we had x-rays taken again. We definitely were not prepared for what we were about to hear. The physical therapy prescribed was not helping Brayden and his curve was now at 42 degrees. The doctor recommended casting but had only had one other case that was casted in a Risser cast as he was not familiar with Early Treatment with Mehta’s specialized EDF casting techniques. Brayden’s doctor advised us to get an MRI to rule out any other issues that may be causing his PIS. He also recommended that we get a second opinion. He was very helpful and answered all our questions.
Within a couple of weeks, Brayden had an MRI done. We were not anticipating anything to unusual to come from this but to confirm his PIS. Nope, we were wrong again. He did not have a chiari malformation yet but there was a possibility he could form one as there were signs of this on his MRI. Luckily this was not anything to be worried about at the moment and was not causing any other issues at that time. The doctor recommended we do routine MRIs every so often to make sure it did not form into a chiari malformation.
After this news, we spent the next couple of days researching for other options for our son. We found the ISOP website and CAST infantile scoliosis Yahoo Group. Both of which were a HUGE resource for us getting the information we needed to make the best decision of treatment for our son.
We found a doctor at Cincinnati Children’s Hospital Medical Center (CCHMC) about 2 hours away from our home. He confirmed his curve was 42 degrees and said Brayden was a perfect candidate for the ET with Mehta’s specialized casting. We were able to get in for casting the next week. It only took him a short while to figure out how to get around with it on. He continued to sleep on his belly as he always had and nothing seemed to bother him.
Brayden is down from 42 degrees to 25 degrees and in his 5th cast currently. Although we miss allowing him have bubble baths, playing in the pool and the squishy hugs, we know that this is just a small sacrifice for improvement to his future health.
Recently, Brayden had another MRI on his brain and upper spine to check the possible chiari malformation. We had great news from his neurosurgeon. This has cleared itself up and there are no possible signs of any chiari malformation. Yeah! We were so excited about this for us and Brayden. We are getting there one step at a time. God is good! All the time!
The last couple of years have been bumpy but we have met many friends along this same path and together we will fight infantile scoliosis thanks to Heather and Dr. Mehta who have helped pave the way for us!
When their beautiful 15 month old daughter, Karleigh, was diagnosed with progressive infantile scoliosis (PIS), Kim Westmiller and her husband had no idea what they were up against. Fortunately, they were able to connect with Heather Hyatt Montoya and the Infantile Scoliosis Outreach Program (ISOP) for guidance, support and answers. Answers that led them to Early Treatment with Mehta Growth Guidance Casting that involves the application of specialized casts every 8 weeks that allow 3 year old Karleigh’s spine to actually grow straight. A gentle corrective method rather than invasive surgery and the resulting complications.
Thankful for their daughter’s progress, the Westmillers decided to hold an event that would celebrate Karleigh’s health and success while raising money for ISOP, making sure that support continues for other parents of children with infantile scoliosis.
On October 20, 2013, The Westmillers hosted *Karleigh’s Cause* at Hearthstone Manor in Depew, NY, featuring Terry Buchwald and his wildly popular Tribute to the King (Elvis that is)! The community enthusiastically attended and supported the live and silent auctions raising well over $13,000!
The Westmillers are a powerful testament to Parent Power and their efforts and belief in ISOP are truly an inspiration. Our deepest thanks to you and Karleigh, as well as your amazing community, including the many event sponsors and volunteers, for envisioning Karleigh’s Cause and making it a huge success. Thank You!
When their beautiful 15 month old daughter, Karleigh, was diagnosed with progressive infantile scoliosis (PIS), Kim Westmiller and her husband had no idea what they were up against. Fortunately, they were able to connect with Heather Hyatt Montoya and the Infantile Scoliosis Outreach Program (ISOP). Through Heather and ISOP, they found answers to their questions and the resources that led them to Early Treatment with Mehta Casting. These specialized EDF casts are applied every 8 weeks and continue to have a straightening effect on 3 year old Karleigh’s spine.
Thankful for their daughter’s progress and wanting to give something back, the Westmillers decided to hold a special event that would celebrate Karleigh’s amazing success and also help raise money for ISOP so that other parents of children with infantile scoliosis could also access the kind of help and resources that they had received.
On October 20, 2013, The Westmillers hosted the first ever, Karleigh’s Cause, at Hearthstone Manor in Depew, NY. The surrounding community rallied around Karleigh’s Cause by attending the event, which featured Terry Buchwald’s, Elvis-inspired, Tribute to the King, as well as live and silent auctions to help raise money for ISOP. In total, the event raised nearly $14,000 for ISOP!
Karleigh’s parents are a powerful testament to the steady devotion and determination it takes to navigate the many health options and difficult decisions they faced upon learning of their daughter’s potentially fatal condition. Also impressive, is the selfless approach and tireless effort they put into making Karleigh’s Cause a huge success, ensuring that other families of children facing similar circumstances will have the needed resources, support and opportunities for treatment that ISOP helps provide.
Thanks to you and Karleigh, and the overwhelming support of your community, event sponsors and volunteers, Karleigh’s Cause was not only an amazing success but truly inspirational.
On behalf of the Infantile Scoliosis Outreach Program (ISOP) and the many families and children who will benefit from your generosity, we say, Thank You!
October, 2013 – Karleigh’s Cause – A Community Success!
When their beautiful 15 month old daughter, Karleigh, was diagnosed with progressive infantile scoliosis (PIS), Kim Westmiller and her husband had no idea what they were up against. Fortunately, they connected with Heather Hyatt Montoya and Infantile Scoliosis Outreach Program (ISOP), they found answers and resources that led them to Early Treatment with Mehta’s Growth Guidance Casting (MGGC).
These specialized casts are applied every 8 weeks and continue to have a straightening effect on Karleigh’s spine. Overjoyed with their daughter’s progress and wanting to give something back, the Westmillers founded Karleigh’s Cause! This family event was a celebration of their daughter’s success and a fundraiser for ISOP.Karleigh’s Cause was held October 20, 2013 at Hearthstone Manor in Depew, NY. The community rallied behind this young lady in full force with a full house in attendance to experience Terry Buchwald’s Tribute to the King, bid in the live and silent auctions, and generally have a blast! In total, the event raised nearly $14,000 for ISOP! The Westmillers navigated a confusing array of health options and made some tough decisions in the face of their daughter’s potentially fatal condition. Let’s just say that they’re a true testament to PARENT POWER! It was important to this family that other parents of children with PIS could access this priceless resource.We can’t say enough how grateful we are for all of your efforts that contributed so successfully to Karleigh’s Cause and to ISOP. Your gift allows Heather to continue to champion straight spines for other children in Karleigh’s situation. The overwhelming support from your community created an event that was an amazing success and truly inspirational. From the bottom of our hearts, thank you.
Our daughter, Olive, was born on September 22, 2010 at 3:46pm. She was full term with no complications, aside from the umbilical cord being around her neck right as she came out of the birth canal. This was cut immediately and there were no issues following. While this was scary, we do know that the cord was not around her neck for long, as her heart rate was consistent all throughout the labor. Olive has had a very healthy childhood thus far with only a few bouts with allergies and ear infections. She has met all of her developmental milestones and is a very happy and outgoing child.
When Olive was about 3 months old we noticed that she seemed to favor leaning her head to one side, so we started propping her head up with a rolled cloth when she was sleeping in her carrier or sleep positioner. At 4 or 5 months we noticed that her back seemed to have a bit of a curve to it and we asked her pediatrician about it. We were told not to worry, that it would straighten up on it’s own.
At about 6 months, we noticed that as she was sitting up, her ribs would stick out further on one side than the other. Once again, we were told it would straighten up on it’s own, but we requested that our pediatrician refer us to an orthopedic doctor.
We got in to a doctor at Orthopedic Associates here in OKC in early August 2011. They took an x-ray of her there, but since she was not yet standing, we had a hard time getting a good look at her spine. They ended up having me “dangle” her in the air, which we now know was stretching her spine out and not giving an accurate look at the curvature. The doctor there told us that 80% of the time Infantile Scoliosis corrects on it’s own, but that he would recommend us to see an Orthopedic Surgeon in 4-6 months. We went ahead and scheduled the appointment with a surgeon at OU Children’s Hospital for December 6, 2011, wanting to get the appointment in on 2011 insurance.
At the appointment on December 6, they were able to do a standing x-ray of Olive’s back that showed her curve to be at 53 degrees. The doctor said that we needed to get her in for an MRI immediately to make sure she didn’t have any other issues causing the curvature. Barring those issues, he wanted us to start casting immediately. We were told that the casting procedure he does was not for correction of the curve, only for maintenance until they can do surgery when she is older. Needless to say, we left in a whirlwind of confusion, sadness and hopelessness.
We immediately got online and searched for a support group- we had been told that IS is very rare, but were hoping that someone out there could give us some encouragement and advice. We found both at the ISOP website, where we learned for the first time about Dr. Mehta and her IS casting technique. We immediately got on the message board there, and were connected with two families in Oklahoma who had children with IS. We have connected with both of those families- Jason & Hollie Lee (Jonas’ family) and Cyndy McKinney (Londynn’s family)- and they all have directed us to Salt Lake City Shriners Hospital, and specifically to Dr. Jacques D’Astous. We applied to SLC Shriners, and in a whirlwind of events we ended up getting an appointment for Olive to be casted just 3 days after submitting our application. We were on a family vacation at the time and ended up leaving the rest of our family and flying to all the way to SLC, not knowing at all what we were getting into!
At Shriners, they did another standing xray and found her curvature to be 73 degrees- a big jump from what it had been just a few weeks prior at the Dr. back home. Dr. D’Astous also did an xray where they held Olive’s head and feet and pulled her in opposite directions, to show how flexible her spine was. In this xray her spine was able to straighten to 25 degrees, which was a very good sign! They did the first cast and were able to get her spine to around 29 degrees in the after cast xrays- how amazing!!
We returned home and adjusted to life in the cast- no more baths or swimming, and we had to learn to be extra careful while eating, drinking, diapering, etc, to protect the cast. Olive had just learned to walk unassisted a few weeks before she was casted, so it was a BIG learning experience after the cast. She could no longer walk, sit up, stand up, roll over, etc, on her own. She just laid on her back and it broke our hearts! When she did get up and walking, she would fall easily and we were scared for her poor little head- we even considered getting a helmet for her in the first few weeks. Thankfully, though, after a few weeks she was able to build muscles that got her up on her feet and falling less often!
We’ve since had 3 more casts and are currently in our 4th cast. The 2nd cast kept us at the same 29 degrees, the 3rd cast got her down to 27 degrees and the 4th cast has her at 19 degrees! They are considering bracing after a few more casts, but they really think that they can cure her and bring her all the way down to 0 degrees!! We are so thankful to ISOP & Heather for pointing us in the right direction- our prospects here in Oklahoma City were not good, and had we not found Salt Lake City Shriners Hospital and Dr. D’Astous, Olive’s future would not be nearly as hopeful as it is now.
Picture 1- Olive, 14 months, before casting
Picture 2- Olive, 14 months, in first cast at Shriners Hospital
Picture 3- X-rays comparing before cast 1 (right) and after cast 1 (left)
Jake was diagnosed with infantile scoliosis at 3 ½ months old when an x-ray was taken to rule out pneumonia. My maternal instincts, however, told me something was not quite right before that. While holding him in my arms, burping him, and bathing him, I could feel that his little spine was bent. But I told myself that I was being paranoid–that he was just a baby he and just wasn’t very strong yet. The x-ray that confirmed our fears showed two curves: a right thoracic curve that measured 20° and a left thoracolumbar curve at 19°. Our pediatric orthopedist informed us that about 85% of infantile scoliosis cases resolve themselves, and told us to “wait and see.” Three months later, our next appointment with him showed promise. Or so we thought. His curves measured 20° and 14° this time, and we were confident that he would resolve, as was our doctor. Four months later the curves measured 26° degrees and 13° degrees. We passed the 25° threshold; it was time for treatment. The doctor recommended a brace to be worn 23 hours a day, and we decided to seek a second opinion.
This is where our research began. Thankfully, we found InfantileScoliosis.org on our first attempt to gather information. We were introduced to the idea of early treatment with serial casting as gentle treatment for Jake’s crooked back, and the video “A New Direction” with Dr. Min Mehta provided by ISOP (Infantile Scoliosis Outreach Program) changed the way we felt about scoliosis. It gave us hope. We were armed with information to take to our next appointment with a new pediatric specialist. This doctor measured the same x-ray (from the first orthopedist) at 24° and 18°. He told us he was not concerned about the severity in degrees, but the rotation of the second curve worried him. This doctor, too, wanted to “wait and see,” but we were afraid of progression. We had to convince him to brace Jake.
Jake was 13 months old when he had his MRI to rule out congenital abnormalities. The following week he was put into his first TLSO brace, which was to be worn part-time at night. We wanted full-time brace wear, but the doctor didn’t agree. One month later, the in-brace x-ray showed the first curve was nearly straight and the second curve was in the 30’s. This was the highest it had ever been, and we were scared silly. How could a curve progress that much in only two months? Our doctor told us to stay the course, and he’d see us again in five months. We argued that this was too long to wait, but he was adamant. We left there scared and confused.
In the meantime, I joined the online CAST Support Group and was learning more from experienced parents there, than from our own doctors. I read a lot of good things about the good people at Shriners Hospitals helping small children and getting great results with early treatment. We decided to send all of Jake’s x-rays and medical history to the Shriners Hospital in Erie, PA., to ask for a professional opinion from doctors who specialize in progressive infantile scoliosis. Their medical team agreed with our second orthopedist: the rotation of Jake’s second curve was definitely “concerning,” although they weren’t sure whether Jake was a true case of progressive scoliosis. They invited us to participate in the ETTP (Early Treatment Trial Project) in November, 2005, where we would meet Dr. Mehta and get her opinion about Jake’s condition. That same week, ISOP also invited us to participate! We felt it was meant to be.
Our experience at the ETTP was awesome! We got to meet several of the parents we had “spoken” with on the CAST support group. We were also introduced to Jake’s current orthopaedic surgeon, and we had the opportunity to have Jake examined by Dr. Mehta. X-rays taken there showed his curve had decreased 5° to 28°. The brace was working. Her opinion: if we were to continue bracing, it should be worn 23 hours a day. Yes, Jake was a candidate for early treatment with serial casting as well, if that was what we wanted. I asked many questions in relation to Jake’s scoliosis, and the conclusion was that Jake was in the gray area: his x-rays weren’t conclusive one way or the other. Dr. Mehta was the third doctor to tell us she wasn’t 100% sure whether Jake had progressive scoliosis or resolving scoliosis. We felt very discouraged. We were hoping someone could definitively tell us the right path to take. Instead, what we learned is that Jake, his back, and his x-rays refused to be “put in a slot.” We learned that every case of scoliosis is unique to the child.
So the doctors put the decision in our hands. Did we want to continue bracing, or did we want to start casting? We agonized over what to do and weighed the pros and cons of each. Our doctor told us that, yes, the brace was working. But would it continue to do so? He assured us he could control the scoliosis and address the rotation better with a cast. Our greatest fear was to miss the precious window of rapid growth during the first two years of life, and Jake was already 15 months old. This fear, coupled with our doctors confidence, led us down the early treatment casting route. We are happy to say that we have not once regretted our decision. We could not believe how quickly Jake adjusted to his cast–he was his normal, happy, energetic self within days!
Our doctor was impressed with Jake’s progress after just one cast. Jake went from 28° before the cast to 8° out-of-cast. This was definitely a testament to early treatment: help the children while they’re young, before their curve(s) grow too large and become impossible to control. Our son is proof positive. After only two subsequent casts, he is now in a modified TLSO brace fashioned after the EDF (elongation, derotation, flexion) casting technique. Out-of-brace he is at 10° and 6° with zero rotation. (His curves keep changing and moving; he now has two curves again.) In-brace he is around 2° and 6°. Jake will soon be two years old; his period of rapid growth is nearly over. We cannot express how fortunate we feel to have seized the opportunity to use this growth when we had the chance.
We’re not sure how long Jake will be in his brace, but we hope and pray it will help keep him where he’s at. We will make an appointment soon for an echocardiogram. His geneticist has ruled that he has some sort of mild connective tissue disorder, and she is running tests to confirm which one. We believe (as do other parents on the support group) that scoliosis cannot be idiopathic. Something has to cause it. In Jake’s situation, was it his connective tissue disorder? Was it intrauterine molding? Was it postural? Or a combination of all three? More research needs to be done. Maybe if we learn the answers, we can learn how to stop further progression. Meanwhile, early treatment with serial corrective plaster casting will continue to be a necessary and superior corrective solution for infantile scoliosis.
The past 20 months seemed to have moved in slow motion on a road that was sometimes bumpy, but the journey has been rich with blessings. We will forever be indebted to ISOP, the organization that helped to educate us and champions for all our kids tirelessly, to Dr. Mehta for bringing her care and early treatment expertise to this country, to the compassionate team at Shriners Hospital in Erie for always doing whatever it takes, and to Jake’s orthopaedic surgeon, who “straightened out” our little boy and is just as excited about it as we are!
Thank you for reading Jake’s story. If you have any questions about his journey, please contact me at jviv314@yahoo.com.
Sincerely,
Jennifer
Jake’s mom
Update on Jake March 2008
Jake only wore his brace for three months before growing out of it in September of 2006. We’ve had x-rays approximately every six months. His most recent x-ray in February 2008 was taken after nearly a year and a half since we stopped treatment. He has a 3.8 degree curve with minimal rotation. Our Ortho is happy with this progress as Jake (now 3 1/2 years old) has grown at a phenomenal pace of almost 6 inches in the past year! Our course of action now is to continue to monitor his spine frequently; his next x-ray is scheduled for one year.
Seattle, WA – Our son Jake was about three months old when an X-ray revealed he had a 22-degree curve of his spine. We saw an orthopedist, who ordered an MRI and a CAT scan to be done under anesthesia. All results were negative and we were told to wait and see if the curve would resolve on its own. It didn’t. We went in for a second X-ray when he was nine months old, and his curve had already progressed to 45-degrees. His orthopedist recommended that we put him in a brace that very day and sent us to the orthotist (brace specialist). They measured him right then for the brace, as he screamed and cried. While this was happening, I asked how many infant braces this team had done? The answer was, “once.” That moment changed my life. My instinct told me we were at the wrong place for my son.
My husband and I did some research and found ISOP (the Infantile Scoliosis Outreach Program), and through them, found facilities that practiced the proven, Early Treatment Mehta Casting Method. I called Shriner’s Hospital in Portland, OR the next day and booked our appointment.
I then called Children’s in Seattle and cancelled the brace that was being made for Jake, confident that we had finally found the solution we had been praying for. We are so grateful to ISOP and its Founder, Heather, for all the advice and help throughout this process.
We arrived at Shriner’s in Portland anxious to get the casting underway; he was 14 months old and had just begun to walk. We were treated so wonderfully at Shriner’s and are forever grateful for the opportunity to have the early treatment performed. The nurses and doctor were so amazing and his casting went beautifully.
By the end of the first day he was walking around and by day-two, he was bending over to pick things up – no problem! It was incredible to watch our resilient and brave little boy, as he was learning how to walk and sit up all over again. Jake went from 50 degrees to 15 degrees in his first cast, which was amazing!
During our last visit to Shriner’s in Portland, his doctor called while Jake was under anesthesia to tell us that Jake’s curve was at 0 degrees! We were shocked and pleased as his doctor advised us to have him molded for his temporary, follow-up brace. He has been in a thin fiberglass brace – similar to the look of his casts – for 81/2 weeks now.
Every family with a child suffering progressive infantile scoliosis has its own story and journey to share. Most are not so happy. For the lucky among us, there is ISOP and Dr. Min Mehta; the hope they inspire; and the early intervention that allows our kids to lead happy, healthy active lives.
Maintaining skin integrity while your child is in a cast will keep them comfortable and reduce the risk of skin problems and irritations.
The “Flossing” process is recommended for children in casts as an effective way to slough off dead skin and prevent potential skin issues. The material used to floss is a basic pair of nylons and is recommended for children with no skin issues.
Watch a Video of River’s Mom performing the Flossing Technique
Cole was born at 36 weeks gestation as a healthy and happy 4.5 lb. baby on March 9, 2005. He has a fraternal twin brother named Jack who does not have any signs or symptoms of infantile scoliosis. At around 4 months of age, we noticed that Cole’s chest wall seemed to protrude quite a bit. We didn’t think too much of it, but at his 6 month pediatrition check up we pointed it out to the doctor. She turned him on his stomach, and we then noticed a few small folds on the right side of his back. She immediately referred us to a pediatric orthopedic surgeon who specializes in scoliosis.
We were able to see him at Cole’s 7 month birthday. An x-ray was taken which revealed a 48 degree left thoracic curve with the RVAD estimated around 52 degrees. The next step was the MRI to rule out any congenital issues. Cole was officially diagnosed with idiopathic infantile scoliosis. The orthopedic surgeon said to come back in 3 months to see if it was a progressive curve and that we would most likely be facing years of bracing, surgeries, and eventual spinal fusion. We were devastated.
We were not satisfied with waiting 3 months, and we turned to the internet for more answers and information. We just new there had to be something less invasive than surgeries and wanted to seek help sooner than 3 months.
Within a few days of Cole’s diagnosis we began reading about early treatment and found a contact number for ISOP. A few weeks later, ISOP invited us to the second Early Teatment Trial Project at Shriner’s Children’s Hospital in Erie, Pa. The timing, location, and treatment was amazing. We felt so blessed and jumped on the chance to have a less invasive, simpler, and less time consuming option for Cole and his future.
At the time Cole was the youngest baby to have ever participated in the ETTP with Dr. Mehta. He was 8 months old when his first cast was applied. The results of his treatment are as follows:
November 10, 2005 (1st cast):
-Before cast: 48 degrees
-In Cast: 28 degrees
-RVAD in Cast: 34 degrees
Cole is now 17 months old and in his 5th cast. He is walking, climbing, talking, and keeping up with his twin Jack. The casts have not held him back at all. We are told that Cole will have 1-2 more casts, and then the bracing process will begin for 6-12 months. By the time he is 2 1/2, we hope to be done with the majority of his treatment. And the best part is we have avoided surgeries, growing rods, and spinal fusions.
Thanks so much to Dr. Mehta and her dedication to these small children. Thanks to ISOP who has dedicated so much time and effort in educating parents and doctors on the benefits of early treatment for progressive infantile scoliosis, and thanks to Cole’s doctor, at Shriner’s Children’s Hospital, Erie, Pa., for learning about early treatment and helping Cole be a happy, healthy scoliosis free kid.
If you have any questions, please feel free to contact me at: michelle_r_baird@yahoo.com
After torrential rains in Fayetteville, NC, early Saturday morning the clouds parted and the perfect day for a 5K run unfolded. At Honeycutt Park, it was a run Straight to the Finish in support of the work of the Infantile Scoliosis Outreach Program (ISOP), a program of Ability Connection Colorado.
50 runners preregistered online and day-of registration began at 7AM to welcome an additional 7 participants (weather reports may have scared some folks away). All registered runners and 1 Mile walkers received a beautiful green ISOP t-shirt and a sincere thank you from 5K race Founding Mother Rachel Jacobs who was busily preparing the site for the event. Rachel’s young daughter Ella has a spine growing straight thanks to ISOP and Mehta Casting! And this race is her way of giving back to ISOP and Heather Hyatt Montoya for providing life-changing resources for the Jacobs family.
Diamond Dust played courtesy of the Cape Fear Music Center
There’s nothing like an early morning concert to set the tone for a great race! Diamond Dust, an all-girl, all-teenager band from the Cape Fear Music Center was on hand to entertain the racers as they geared up to run. Playing their version of rock classics from Heart to Joan Jett, it’s safe to say that these ladies earned some new fans and got our athletes pumped up.
At 8:30AM the whistle blew and the runners were off on a beautiful 5K (3.1 mile) course that wound through the beautiful and quiet neighborhoods behind Honeycutt Park. The first runner finished in just 18 minutes and remarked “Wow – what a great course! If you do this again next year, I’ll be here.” With that he handed the ISOP t-shirt to his 7 year old daughter/biggest fan and they headed out to enjoy the rest of their day.
Oden , the youngest finisher of the 5K is congratulated by Sweet Frogs
All the racers finished in good time and great spirits. Two large Sweet Frogs greeted finishers with water and energy bars to replenish their efforts as well as Sweet Frog coupons.
First-time 5K racer Carmen traveled over an hour to Fayetteville for the race and was beaming as she crossed the finish line. Oden was our youngest racer at 3 months (pictured below celebrating with the Sweet Frogs!) and longtime runner Gregg was our most mature participant at 74 years young.
The proceeds from the Inaugural 5K Race Straight to the Finish will allow ISOP to continue training physicians through hands-on tutorials in Mehta’s Growth Guidance Casting — the only noninvasive cure for progressive infantile scoliosis.
Thank you to The Jacobs Family and darling Ella for your compassion and drive.
Brooke was born on July 7th, 2001. At 4 months old , intuition told me something was not quite right.
At 6 months old, I noticed that her back was curved slightly. My father and her father both agreed.
I called the pediatrician and was seen the next day. At the appointment, we asked about scoliosis. We were told no, but to ease our minds an x-ray was taken. They called later that day to say that Brooke indeed, had scoliosis. At the time her curve was measured at 27 degrees low thoracic, and 20 lumbar.
We were told then to see a specialist. We did, at our local Children’s Hospital. This hospital insisted on doing more x-rays of their own. These films were unnecessary, and revealed the same measurements as before.
The doc looked at her back, and suggested that we return for a follow up in 5 months. That seemed unreasonable, but at that time I didn’t know too much about scoliosis..
Within a couple months it was obvious to us, that the curves were progressing.
I called to set up an earlier appointment. She was 9 months old, and not able to completely sit up unassisted.
Another doctor in this hospital ruled out congenital abnormalities, after an x-ray was taken of her head and neck area. No structural abnormalities were found.
More x-rays revealed that Brooke’s curve had progressed to 37 degree low thoracic and 30 degree lumbar, in a couple months. At this time they suggested we get a brace. We could get one at the hospital which was 2 hrs away, or we could contact our local orthotist. We chose the latter, which was also a mistake. They insisted on more x-rays.
The 2nd doctor from our local children’s hospital never recommended a follow up appointment to make sure brace was adequate.
She was placed in her first brace close to her first birthday. They were neglectful on directions, care and tightness of this TLSO Brace.
The brace was not adequate, and they felt that it was not holding her. It was taken to numerous places for adjustments, but never fit well. It was worn 23 hrs a day.
This is when my research began. I joined numerous internet support groups, in effort to learn more.
I told Brooke’s Story and was contacted by Heather. We talked about the ineffectiveness of bracing these small infants/children. Heather recommended casting as a way to maintain Brooke’s curve.
We had Brooke in physical therapy at the time because she still could not sit or stand unassisted. I showed our physical therapist’s Brooke’s x-rays, and they suggested we look into a scoliosis clinic in the same hospital The doctor there suggested an x-ray of Brooke in her brace to make sure it was holding her, and it wasn’t.. She was then measured without the brace and this revealed that her true curves were 55 degrees low thoracic, and 45 lumbar.
I knew as a mother that I needed to act fast. I wanted another opinion, so I made yet another appt at another reputable children’s hospital in Pittsburgh, PA. This doc took more x-rays with and without the brace. He felt that I was not putting the brace on tight enough, so he tightened the brace and measured her at 25 degrees. He also stated that he was not impressed with this particular brace. He said that her scoliosis would progress with her growth, and that we should just “wait and see.”
In Jan 2002, we had an appt with the Shriners in PA. They made a new brace for her in 2 weeks. They also predicted cast’s, and a halo in her future before surgery in effort to maintain her curves and prolong surgery for as long as we could.
A follow up appt with the Shriners in Erie PA. was made in a month. The doc thought the brace was effective, and wanted to see Brooke again in 3 months.
Before her next appt., I was contacted again by Heather. She informed me of her recent connection with Dr. Mehta. She sent me the video, “A New Direction.”
Upon watching the video, I knew that I needed to give serial corrective plaster casts some consideration. No one had ever given us any hope before. WAS THIS FOR REAL?
I immediately presented the video to her doctors at the Shriners. Her doctor watched it and called me back. He said that he was fond of Dr. Mehta’s work, and that he was willing to put a plaster cast on Brooke, if that’s what we desired!
Although, at our next appt. her curves were measured 10 degrees lower. We were so happy! We just knew her curves were going to get better at that point. We were given a little hope, and we ran with it. But, in the back of my mind, the video continued to replay.
Meanwhile, Tawney, (Tyler’s Mom) called to inform me of his wonderful progress in his first cast..
I was excited for her, but was also confident that Brooke was getting better, so why torture her during the summer in a cast? Not to mention, she was in aquatic therapy and loving it.. I knew it was benefiting her at the time, and her doctor agreed.
An appt was made in 6 months, but that was not soon enough. The brace wasn’t fitting well, and we needed another approach.. We were seen again in 4 months, and it was decided that the brace was not holding.
I knew then that it was time for a cast. Her doctor agreed, and Brooke’s first plaster cast was applied 2 weeks later, at age 2yrs and 4 months old.
We were admitted to the hospital on November 4, 2003, the night before her first cast was applied. She was measured at a 47 low thoracic, and 43 lumbar. .In the cast, she was measured at 17 degree low thoracic, and 5 degree lumbar.
We went home that evening. We were so exhausted.
Unfortunately, Brooke was reacting to anesthesia, and then developed bronchial asthma. Needless to say, the first 2 weeks were quite difficult.. Although, we knew most of her discomfort was due to the asthma.
Within a couple weeks she had completely adjusted to her new cast.
Our follow up appt. was one month later, and the standing x-ray revealed that she had settled to 25 degrees, in the cast.
We had to schedule an earlier appt, because she had grown so much in a couple months. The cast was sawn off, and her 2nd cast was applied. Her doctor was able to get her down to 12 degrees in this new cast!
She adjusted to this new cast even quicker than the last.
We are now scheduled to go back at the end of March.
I would like to give special thanks to Dr. Min Mehta for dedicating her life’s work to the treatment of our children.
I would like to thank Dr. James Sanders for applying the casts when no one else would.
I would like to thank Heather Hyatt and The Infantile Scoliosis Outreach Program for giving me the educational material I needed to make the best choices for my daughter Brooke.
My daughter’s curve correction would not have been possible without the dedication of these people, and for that I am eternally grateful.
Thank you for reading our story, and feel free to contact me with any questions regarding Brooke’s care.
After two years of extensive research, I was finally able to locate the only person on the planet willing and able to help my child. Unfortunately, he lives in France. Luckily, I made contact with him before he retired in June 2000. His recommendation was for a procedure considered experimental, and not commonly practiced in the U.S. It consists of halo traction, a specialized, two-piece, adjustable plaster cast with turnbuckles, and Bi-Pap breathing exercises. The combination procedure was performed on October 2, 2000 on 2 ½ year old Olivia & 3 1/2 yr old Breann at the Shriners Hospital in Salt Lake City, Utah.
This traction therapy/experimental procedure took three months. So far, we are extremely happy with the results. Olivia entered the hospital with a 96º thoracic curve. One month later, the curve was at 45º. The goal now is to maintain the curve, she is currently in a plastic brace with neck support. it’s a lot of hardware, but it allows removal once a day for the skin to breathe, and the alternative exercises we’ve chosen to stretch & straighten her spine, i.e. inversion table, hanging rigs, pilates, yoga and more. Details on these and other disciplines will follow, but it’s important to note now that they strengthen muscles that are not used while in a Risser Cast the other 9-11 months of the year. My research indicates Olivia’s curve will revert back to 96º within 1 ½ -3 years if alternative solutions are not found. Bracing without neck support has proven to be of no significant benefit for this type (thoracic) infantile scoliosis and certainly not at Olivia’s age.
Chronological History
Following Olivia’s birth, an intern who examined her heard a clicking in her left hip and asked seven other doctors to examine her. They all concurred there was nothing wrong with her hip and refused my request to give her an x-ray. They stated they don’t expose newborns to unnecessary radiation. Five months later, while giving Olivia a back massage, I noticed that the left side of her back seemed to be a little more muscular than the right. I immediately took her back to the hospital where she was delivered. They intimated that she was lazy and only wanted to use one side of her body, therefore, we should move all activities to the opposite side of the room to make her use those other muscles. This was tried for a few wasted hours. She had always used both sides of her body and I didn’t believe the diagnosis. Instead, I took her to Children’s Hospital in Denver where they took x-rays and immediately diagnosed Infantile Scoliosis. At this time her thoracic curve was measured at 39º.
At my insistence, an x-ray was taken of her hips and it was determined her left hip had been subluxed since birth thus favoring (but still using) the one side. Her hip was reset and she was placed in a spica cast for one month.
This was followed by a hip brace for three months (while the spine continued to curve), but I was told the hip must be aligned first, then the TLSO brace worn in order to attempt correction or at least maintenance of the spine. She was then fit for a TLSO brace that was unsuccessful in maintaining her curve. This meant continued deterioration and ultimate fusion of her spine before her torso would be fully-grown. It meant certain lifelong deformity with severe respiratory problems.
Frustrated with the doctor’s inaction to stop this progressive curvature of the spine, my research on Infantile Scoliosis began. I took Olivia to at least 20 Orthopedic doctors who’s specialty was Scoliosis in our state (Colorado). All of them agreed with the diagnosis and treatment except for one doctor who said that Olivia needed serial corrective plaster casts. She indicated that this treatment probably wouldn’t be available to us in the U.S. because doctors here consider this practice archaic and ineffective.
I began sending Olivia’s x-rays to most major Children’s Hospitals in the U.S.
I then began sending them abroad to France, England, Scotland and Holland. I either received no response from the U.S. doctors or their response was to advise me to keep Olivia in the TLSO brace and “hope for the best.” All the doctors abroad agreed that bracing without neck support has not been shown to be of significant benefit for this type (thoracic) infantile scoliosis, and certainly not for a child Olivia’s age.
I presented this information to all of her Colorado doctors and they insisted that serial corrective plaster casts were ineffective, barbaric and an archaic practice. I then made the decision to raise money to live in France where I knew of a doctor who could help us. I was determined to speak to him personally. Fortunately, I was able to obtain his home address and immediately began sending the x-rays and medical information to him. He called me at home and once again confirmed that Olivia needed serial corrective plaster casts with neck support. Again, her Colorado doctors didn’t agree with this recommendation.
Olivia’s Colorado doctor at this time was planning a trip to France for a spinal convention and was able to confer with this French doctor about the right course of treatment. Upon his return, his mind was changed.
I then re-contacted a doctor at the Shriners Hospital in Salt Lake City with whom I had been corresponding all along. He informed me that this French doctor would be in Salt Lake City in June 2000 before he retired and that he would try to set up an appointment for Olivia. We met him at Shriners where he examined her and conferred with the doctors at Shriners, who agreed to treat her, per his recommendations.
The other recipient of this procedure, also a Coloradoan, 3 1/2 year old Breann, curve has improvement from 69 degrees to 28 degrees.
The above successful results occurred because Dr. Jacques D’Astous was willing and committed to try a therapy not commonly done within the U.S. There ARE alternative solutions besides fusion for this type of scoliosis in the U.S., and he alone was able to provide one. We are eternally grateful and indebted.
October 2003 Update
I am sorry for not having updated this site sooner.
Much has happened since the last update. Like my introduction to orthopaedic spinal surgeon, Dr. Min Mehta.
Through my relationship with the Scoliosis Association in the United Kingdom, ( S.A.U.K.), I was introduced to Dr. Mehta who has successfully treated a large number of infants with progressive infantile scoliosis using serial corrective plaster casts.
Dr. Mehta does NOT “wait and see,” how large the curvature is going to increase before applying a cast, but rather applies the cast immediately after completion of necessary exams to confirm the diagnosis of a progressive scoliosis.
This immediate approach to treatment has resulted in successfully straightening the spines of numerous infants and young children. She has followed the progress of her patients for over 10 years, and has found they continue to remain straight.
I have a video produced by Dr. Mehta, her foundation ARISE, U.K. and the parents of children whos spines have been improved or completely corrected.
If you would like a copy of this tape, please contact me at, heather@abilityconnectioncolorado.org/newsite/infantilescoliosis.com. All proceeds go to ARISE, U.K.
The first Infantile Scoliosis Outreach Program ( ISOP), in America is now officially being developed. “My relationship with Ability Connection Colorado now gives ISOP the opportunity to fundraise. I will keep you aprised of events on a regular basis.”
Thanks for your emotional support in the past, and I look forward to our continued communication through the new list serve, “C.A.S.T.” , (Casts As an Alternative for Scoliosis Treatment), e-mail, and telephone.
Now, for an update on Olivia.
On September 25, 2003 Dr. D’Astous applied her “winter,” cast. She was able to spend the entire summer in a removable brace, which made for a great summer!! She continues aquatic therapy during “cast-off,” time, and exercises everyday.
Her thoracic curve is currently around 67 degrees. A far more livable degree than 96 , which is where the curve was exactly three years ago!!!!!!!
We are all very grateful and happy with her progress, and will continue our research into the future.
Sincerely.
Olivia’s Mom
Olivia’s Update – November, 2006
In an effort to maintain her severe curves, Olivia wore casts and braces until she was eight years old. At that time, her doctors determined casting/bracing would no longer be enough help for her tenacious curves, and recommended a more aggressive care plan. Because her largest curve had returned to 100+ degrees, it was determined that halo traction would, once again, be her best option. Olivia was placed into her second halo on January 15, 2006, and was hospitalized for about two months. Her first halo, in 2000, bought her six years of precious growing time, so we were looking forward to the second episode of non-surgical correction she was likely to achieve with the halo. In further support of the halo traction procedure, we had recently discovered and researched a new surgical procedure for which halo placement was a prerequisite. If Olivia was to qualify for this new procedure, the halo would first have to decrease her curves enough to make the procedure viable.
This new procedure, called the dual-hybrid version of the Vertical Expandable Prosthetic Titanium Rib (VEPTR), had only recently been developed by an orthopaedic surgeon in Salt Lake City, UT. The dual-hybrid VEPTR is a surgical procedure that consists of two rods that are made of titanium, are adjustable, and are placed on the outside of the ribcage. They are attached to a set of top ribs and to the pelvic structure on the iliac crests.
It is intended to be a temporary option, to help Olivia maintain her current degree of 60, until she reaches skeletal maturity. At that time, the devices will be removed prior to her definitive procedure. The hybrid is considered internal splintage, and must be adjusted surgically as the child grows, approximately every six months. We decided to pursue this new option for many reasons. First, it was recommended by our trusted orthopaedic surgeon. Second, the implanted hardware doesn’t touch the spine directly.
Olivia’s initial implantation surgery took about an hour, and recovery took about a month. It was a very difficult process, but the result was worth every minute of pain! Olivia had grown four inches by the time both procedures were completed. We had to go shopping for a whole new wardrobe! In early September 2006, Olivia underwent her first hardware expansion—a minimally invasive procedure from which she recovered quickly.
All in all, we are very pleased with Olivia’s progress. She is living a new life after undergoing these procedures. She attends school full-time, and does everything a typical kid does. She is a really fast runner, and she is in her fourth year of piano lessons. She is in the process of picking out her annual piano recital piece, and will probably choose a song composed by Alicia Keyes (her favorite artist).
My daughter, Madison, was diagnosed with infantile scoliosis at the age of 6 months. All of the initial information I received from her treatment team involved countless surgeries and no promise of real correction. Through the ISOP website I was able to connect with other parents who were experiencing the phenomenal success through a series of EDF jackets. After more research and several conversations with Heather Montoya, I opted to seek this same procedure for my baby.
We began our EDF journey at a Shriner’s Hospital. Madison is now completely corrected. She leads a very active lifestyle participating in gymnastics, ballet, and soccer. She has remained corrected; without further treatment since 2005. Without this innovative procedure, the level of deformity she would surely be at, would not allow her this quality of life. I am eternally grateful to ISOP, Heather, Shriner’s, and Dr. Mehta.
Awarding this grant to ISOP will offer countless other children the same opportunity to experience this same success. Heather’s vision and perseverance to educate the globe in this gentle, effective treatment is unsurpassed. There must be a continuation of education, not only in the simplistic diagnostic approach and awareness campaign to pediatricians across the country, and around the globe, but certainly in the process of early treatment.
Madison was born full term by cesarean section on August 26, 2003. At birth, her pediatrician noticed a click in her left hip. An orthopedist was called in, and she was immediately placed in a Pavlic harness. She wore this removable brace 24/7 for three months. Under no circumstances, we were told, should it be removed. Finally, when she was three months old, I gave Madison her first bath and noticed the hump in her ribs.
I took her back to the same group of orthopedists, who actually specialized in pediatric scoliosis, and was told that there was nothing wrong with her spine. They suggested that the Pavlic harness had caused Madison to use only the muscles on one side of her body, and that she would need a little time to readjust. My husband returned from deployment when Madison was seven months old, and he immediately noticed her rib hump. This is when we concurred that there was definitely something wrong.
We took Madison to the pediatrician who examined her back with a scoliometer and immediately concluded that she did, in fact, have some type of scoliosis. X-rays confirmed our suspicions. This was March 23, 2004, and her COBB and RVAD both measured 30°. He referred us to an orthopedist he knew personally who specialized in infantile scoliosis. This doctor prescribed a TLSO brace, which Madison wore home that day. In the brace her COBB measured 13°. One month later, her out-of-brace x-ray revealed her COBB at 48° and RVAD at 50°. She wore this TLSO brace 23 ½ hours each day; it could be removed only for bathing three times each week.
At this time, the doctor mentioned that he knew of some great work being done for progressive infantile scoliosis at Intermountain Shriners Hospital in Salt Lake City, and this is when my search began. I spent the entire night on the Internet, and that is when I came acrosswww.abilityconnectioncolorado.org/newsite/infantilescoliosis , which has proven to be an invaluable source of information on the early treatment of progressive infantile scoliosis. ISOP gave us the “A New Direction” video, and I was able to discuss this gentle alternative with other parents who were currently experiencing early treatment with their infants/young children. Within a couple of weeks, we decided to pursue this uncommon option for Madison.
While we anxiously awaited her evaluation appointment at Shriners, our pediatrician sent us for what seemed to be 1,000 tests. Madison had an MRI of her spine, a slit test with an ophthalmologist, a renal ultrasound, and a genetic appointment to rule out a connective tissue disorder. The renal ultrasound led to radionuclide VCUG. She was also referred for an echo cardiogram; however she was cast before we could get that appointment.
Madison’s progress was as follows:
26 May, 2004
Before cast application: COBB 52°, RVAD 40°
After cast application: COBB 21°, RVAD 20°
*Rotation was significantly reduced
14 July, 2004
After 2nd cast application, COBB 14°, RVAD 2°
13 September, 2004
Before cast x-ray, COBB 25°, RVAD 6°
After 3rd cast application, COBB 2°, RVAD 6°
At this casting, we noticed that her rotation had increased and a new compensatory curve had developed.
After 4th cast application, COBB 11°
22 Nov, 2004
Before cast application, COBB 17°, with increased rotation
After 5th cast application, COBB 8°, RVAD 1°
9 March, 2005
Before cast application, COBB 16°, RVAD 3°
After 6th cast application, COBB 5°, RVAD 0°
25 May, 2005
Before cast application, COBB 5°, RVAD, 0°
After 7th cast application, COBB 0°, RVAD 0°
(mold for TLSO made while still under anesthesia)
Madison’s final cast was removed on July 27, 2005. Her COBB was 12°.
This x-ray was taken after she had been cast-free for 24 hours. The previous out-of-cast x-rays were taken within 5 minutes of cast removal.
Madison wore the TLSO until January 2006. She began wearing a new brace January 10, 2006. Recent x-rays show her COBB at 4° and RVAD at 0°. We will begin to wean her off the current brace in March 2006, by reducing the time she wears it by two hours each day, each week. Then, she will wear it only while she sleeps for one month. If new x-rays then reveal that Madison is maintaining her correction, the bracing will be discontinued.
Dr. Mehta, Dr. D’Astous, the entire team at Intermountain Shriners, and ISOP will always have a place in our hearts. We can’t thank them enough for their dedication to our children with progressive infantile scoliosis.
Rylie was born January 29, 2006, full term by cesarean section. She was a healthy 5lb 14oz little girl. Three weeks after Rylie was born my mother brought to my attention that Rylie kept her head tilted to the left. I took her to see the pediatrician who confirmed she had Congenital Torticollis and referred her for physical therapy. At 10 months old the torticollis had resolved, however Rylie still had a very obvious hump on the left side of her back. The physical therapist thought it was a muscle, however I myself had progressive adolescent scoliosis and my gut told me it was not muscle. I scheduled an appointment with a Pediatric Orthopedic doctor at our local children’s hospital. Rylie was 10 months old at the time of her visit. The doctor did x rays with her standing and confirmed that she had Infantile Scoliosis with a left thoracic curve measuring 40 degrees. They recommended we get an MRI to rule out any other anomalies and to confirm it was idiopathic scoliosis. January 2, 2007 Rylie had the MRI which confirmed it indeed was idiopathic scoliosis.
The doctor informed us this was most likely progressive infantile scoliosis due to the degree of curvature and to come back in four months for a follow up. They said at that time we can discuss our options for treatment once they get another set of x-rays. My husband & I were not willing to “wait and see”. That is when I started my search and found ISOP (Infantile Scoliosis Outreach Program). As I read all of the success stories I knew this was exactly what we were looking for, a non-invasive method of treatment.
I immediately joined the C.A.S.T. support group. All members of this group were very helpful as they explained the Early Treatment casting method and the importance of a Mehta trained doctor. We were put in touch with the Shriners hospital in Erie, Pa.
Rylie was evaluated by a surgeon who had been recently trained on the Mehta Method. The surgeon confirmed Rylie was a candidate for the Early Treatment Method and applied her 1st plaster jacket on March 8th 2007. She had an x-ray lying down prior to casting that revealed a 27 degree left thoracic curve with 25 degrees of rotation. In her first cast she had another x-ray showing a 7 degree curve & 7 degrees of rotation.
The rest of the casting went as follows:
2nd Cast May 3, 2007
Out of cast – 20 degree curve / 0 rotation
In cast – 6 degree curve / 0 rotation
3rd Cast July 11, 2007
Out of cast – 17 degree curve / 0 rotation
4th Cast September 6, 2007
Out of cast – 12 degree curve / 0 rotation
My daughters surgeon anticipates this being Rylie’s last cast. We are scheduled to return in November 07. As long as Rylie’s curve has improved to a 10 degree curve, she will be molded for her brace.
We are so pleased with her progress and are forever thankful to the ISOP and the Shriners Hospital Network. They have completely changed our daughters quality of life.
Please don’t hesitate to e-mail me, should you have any questions regarding my daughters progress with this gentle, effective treatment.
Dylan was born in October of 2006. He was born 3 months premature for unknown reasons. I had no complications during the pregnancy, but started dilating and having contractions at 25 weeks. I was put on bed rest for 3 weeks and took terbutaline to try and stop the contractions. At 28 weeks, the labor could no longer be stopped. Fortunately, the doctor had given me corticosteroids a couple days prior to his birth which helped develop his lungs quicker and he had a pretty smooth course through the NICU.
He came home after 43 days in the hospital. We noticed after having him home a few weeks that he held his neck to the right all the time. We mentioned it to the pediatrician and she explained that it was torticollis (a tight neck muscle). She recommended physical therapy. Dylan started seeing a physical therapist in the spring of 2007. She worked on his torticollis as well as helping him to reach milestones, since he had some mildly low muscle tone which was likely due to his premature birth. He also had plagiocephaly (flat spot on one side of his head). It is fairly common in preemies and in children with torticollis.
In May of 2007, he received a STAR band helmet to help mold his head and reduce the flat spot. He wore the helmet for 3 months. In June of 2007, he was just beginning to sit and we noticed that he would slump to the right when he sat. Somehow this came up in discussion when we were seeing his orthotist for the STAR band. The orthotist asked if he could hold him a minute and he felt his spine. He suggested that we get him checked for scoliosis. We asked our physical therapist about this and she felt pretty confident that his spine was straight, but we still followed up with our pediatrician. She also thought his spine seemed straight, but ordered the x-ray as a precaution. Sure enough, the x-ray showed a 16 degree curve.
I immediately started researching infantile scoliosis on the internet and found the Infantile Scoliosis Outreach Program (ISOP). I learned about RVAD (Rib Vertebral Angle Degree) measurement and how it is an indicator for progression and saw the recommendations for getting a MRI done to rule out congenital issues. We were referred to a local orthopedic and he gave us the RVAD measurements and suggested a MRI and an echocardiogram. I also asked about a kidney ultrasound since I had read somewhere that kidney issues could be linked to scoliosis. He thought that was unlikely, but approved it as well. Dylan’s RVAD was only 5 degrees, so he recommended just waiting and watching. This seemed in line with what I had read during my own research, so I felt good about the decision. However, even though all of his tests came back normal, I noticed that the MRI results indicated a 20 degree curve which concerned me since it had only been a couple weeks since the initial x-ray was taken that showed a 16 degree curve.
I called the local orthopedic and he ordered a second x-ray. This x-ray confirmed a 21 degree curve. At that time, the orthopedic recommended a Charleston Bending Brace to be worn at night. I asked the local orthopedic about Early Treatment with casting and he did not recommend it at that time, but I got the impression he had not had a lot of experience with it. I decided to be proactive and schedule an appointment with one of the doctors who believed in Early Treatment with the Mehta style of casting for infantile scoliosis. In the meantime, we went forward with getting the Charleston Bending Brace.
Our first visit with the doctor who had been trained in Dr. Mehta’s method was in October of 2007. Dylan’s x-ray showed a 31 degree curve and while his RVAD was still below 20 degrees, it too had increased. At first, the doctor seemed a bit on the fence on whether to cast him or not, but when I showed him the previous x-rays and how rapidly the curve had progressed, he immediately recommending casting him. Dylan received his first cast the week of Thanksgiving. It took a couple days to adjust to the cast, but soon he was doing all of his normal activities. He continued to receive physical therapy and we went about our lives as usual. He wasn’t able to get in the bathtub or go swimming, but other than that the cast didn’t seem to bother him too much. He was a little delayed in reaching some milestones such as crawling and walking, but is now on target for all of his gross motor milestones.
Every 8-10 weeks we flew up to Chicago for a new cast. Out of the first cast his curve was 21 degrees. Out of the second cast, his curve was 10 degrees. He recently just had his third cast taken off and he is now down to 0 degrees!!!! He is now in a TLSO brace to hold the spine in place. He will wear this brace 20 hours a day for at least the next 6 months. The plan is to follow up with x-rays every 3 months and if he maintains 0 degrees we can take the brace off in 6 months.
Evan was born August 7, 2005, four weeks early, but overall, a wonderfully healthy baby boy. As a mother, I thought that my baby boy was just perfect! I did, however, notice that his ribs did protrude quite a bit on both sides. I attributed this to him being a chunky little boy! A very dear friend of mine discovered at four months old that Evan displayed some characteristics of scoliosis and we referred this concern to his pediatrician.
We made an appointment at Wake Forest University in the pediatric orthopedic department. While waiting for Evan’s appointment, we noticed a progression in his curvature. He slowly began to lean more to his right side in his car seat and swing. Evan was evaluated in November at WFU and was diagnosed with infantile scoliosis. We had SO many questions and felt unsure of the recommendation- to “wait and see” if Evan’ s curvature would progress. As a mother, I didn’t feel comfortable with the options we had been given and began to research.
After reading ISOP’s website, I was determined that Evan needed to have an MRI done to rule out any abnormalities and we had his MRI on 12/31/05. During this time, I noticed that in addition to his body curving to the side, that he had a hard time with turning his head past the midline. We visited a pediatric neurologist and he was diagnosed with torticollis. I was concerned with the difficulty I saw that Evan had moving his head and neck. His pediatrician agreed that he needed physical therapy to help with the torticollis, which resolved around 13 months. After researching and finding the wealth of information that I did on ISOP’s site, I made and appointment at Duke University for a second opinion. It was confirmed in January 06 that Evan indeed had infantile scoliosis, and determined that Evan fell into the progressive type of scoliosis. His MRI showed that his scoliosis was not congenital and that there were no structural abnormalities. At the time, Evans curvature(s) measured at 32 degrees and his RVAD mid 40’s. We shared the DVD that I received from ISOP on the effectiveness of early treatment for progressive infantile scoliosis, and were amazed that all the doctors my son had seen, were recommending bracing or surgery.
We decided to take Evan to Shriner’s in Erie, PA. and he was evaluated in early February. The doctors there agreed that Evan was a candidate for Early Treatment, and on March 14th, Evan was in his first POP (Plaster of Paris) cast. His curvature started out at 46 degrees and his rotation of his ribs was at 64 degrees. Out of his first cast he was 28 degrees with a RVAD of 38. His second cast was applied and he was at 19 degrees in this one! Evans 3rd in-cast measurement was 21 degrees, 4th cast -16 degrees, 5th cast-13 degrees, 6th cast- 11 degrees! What a blessing! Evans doctors say that as long as his curvature(s) dont progress any, after his seventh cast he will be ready for a brace that will be worn 23 hours per day. He is currently in his seventh cast and will be fitted for a brace in March 2007!
Brandon and I are so thankful for these wonderful organizations that have given so much, to my son and my family. They have given us hope, where there was little. The numbers speak for themselves-correction is being achieved for Evan and for many other children across the USA, and abroad. ISOP has given my family and many other families a wealth of information and resources that are invaluable and Shriner’s in Erie, has been a wonderful place to receive Evan’s care. I am in the process of organizing a fundraiser for ISOP and Shriner’s in Spring 07. I want to give back just a part of what was given to us: HOPE.
If your daughter, son, granddaughter, grandson, nephew or niece has a non-resolving case of progressive infantile scoliosis, you have every right to demand the right treatment. Follow the guidelines on ISOP’s website, have all tests done to rule out any abnormalities such as an MRI, order “A New Direction” DVD and arm yourself with all of the knowledge you can. We initially had no hope or anywhere to turn to help our little boy, but thanks to Early Treatment, we had promising options. We had the opportunity to meet Dr. Mehta at the ETTP in Philadelphia, PA in the fall 06, and I felt so very encouraged after her examination of Evan. Thanks to Dr. Mehta’s hard work and dedication, our children are receiving the Early Treatment they need without the need for invasive surgery with such a gentle correction. Evan’s spine has gently been trained to grow straight through the series of 7 casts that he’s had applied. We look forward to the brace in March and time that Evan can enjoy in the bath and pool, but are thankful for the awesome correction we’ve received with the Early Treatment casting process.
Blessings,
Brandon and Jenny
Related Story: Read more about Evan and the bluegrass benefit called HopeFest that was held in April, 2007 and organized by Brandon and Jenny. Click here to read the article.
Our son Evan was born on March 20, 2006. We could not believe how beautiful he was, and there was no missing his gorgeous eyes. We really weren’t aware that anything was wrong with his back until his 4-month regular check-up. His doctor noticed that he had a slight head tilt and wanted to get an x-ray of his neck. Because he was so small, when they took the x-ray of the neck, they also caught a portion of his spine on the film. We were told that he had torticollis, which has since resolved through physical therapy, and what appeared to be infantile scoliosis. This was the beginning of our journey toward a cure.
Evan had an MRI done, and his first visit with a local orthopedic doctor before he was 5 months old. He was diagnosed with idiopathic infantile scoliosis with a curve around 30 degrees. We were told to wait and see if the curve progressed and continued with regular check ups until he was 10 months old and his curve had progressed to 42 degrees. I immediately began searching for any information I could find about infantile scoliosis. This is when I came across ISOP (Infantile Scoliosis Outreach Program) and the C.A.S.T. support group. Finding this information literally changed my family and more importantly my son’s life.
Evan had his first appointment and casting at the Shriner’s Hospital in Erie, PA when he was 12 months old. His curve had now progressed to 49 degrees and he had an RVAD of 20 degrees. He had not taken his first step before the first cast and it only took 2 weeks in the cast and he was walking everywhere. When they removed the cast after 2 months, his curve was measured at 34 degrees (a 15 degree correction), we were thrilled. His subsequent castings and corrections are as follows:
COBB 49°, RVAD 20° Before Early Treatment
Cast #1 Date 3/26/07 COBB 34°, RVAD 11° out of cast
Cast #2 Date 5/29/07 COBB 27°, RVAD 2° out of cast
Cast #3 Date 7/26/07 COBB 22°, RVAD 2° out of cast
Cast #4 Date 10/04/07 COBB 16°, RVAD 2° out of cast
Cast #5 Date 12/04/07 COBB 12°, RVAD 2° out of cast
Cast #6 Date 2/25/07 COBB 12°, RVAD 0° out of cast
Brace Date 4/30/07 COBB 15°, RVAD 0° out of brace
Cast #7 Date 6/16/08 COBB 4°, RVAD 0° out of cast
Brace Date 9/21/08 COBB 3°, RVAD 0° out of brace
Currently scheduled to be in his current brace until July 09
Evan’s physician transferred to Strong Memorial Hospital in Rochester, NY in January of 08 and we continued care there in June of 08. Evan has been in a brace for 6 months now and at our most recent visit we were told that he appears to be cured, but he will continue to wear the brace for another 6 months, to ensure the correction holds. My whole family is extremely grateful that there are physicians out there who are taking the time to learn about this condition and Early Treatment through EDF casting. We are so thankful to ISOP, the C.A.S.T. support group, the work of Dr. Mehta and the wonderful staff and doctors at Shriner’s and Strong Memorial Hospitals. My son most likely will not remember much of being in his casts, but he will forever stand tall because of them.
“Strength does not come from physical capacity. It comes from an indominant will.”
Mohandas K. Gandhi (1869-1948)
My son Finn is the very essence of the word strength. He is also determined, witty, and charismatic. For in his three short years he lives his life with the wisdom of an old soul. He has struggled and he has rallied. His life has not been one of ease but he has blossomed into a thriving, energetic young boy.
Finn was born into my arms on May 31, 2006. I had struggled with Polyhydramnios in my pregnancy that has ballooned my stomach to twice the normal size of a single pregnancy. I went in weekly for the last 6 weeks of my pregnancy for fetal monitoring and at 38 weeks my midwife and physician decided it was time to induce labor. Finn’s delivery was uncomplicated and very natural. We had not known if he was a boy or girl and were overjoyed when the announcement from my midwife was that he was a boy. My daughter Mia, then almost 4 years old, attended the birth and was the proudest big sister I had ever seen. I did notice that Finn was bruised on one side of his face and that he had some difficulty opening his left eye, also that his left eye sat higher on his face than his right eye. I was told that he was a little shifted from the delivery and once the swelling went down all should be normal. His Apgar at 1minute was an 8 and at 5 minutes was a 9.
Hours into Finn’s arrival his muscle tone decreased and he had difficulty with his breathing. He was grunting and was taken to the nursery for oxygen. After three days in the hospital he was released and we went home to begin our life as a family of four. Within days I noticed that Finn sharply tilted his head to the left with his chin sitting on his right shoulder. His position looked so uncomfortable but it seemed very natural to him and when I repositioned his neck he would again rotate it to the side. The next thing I noticed was that his eyes did not move correctly. Even though he was a newborn he had absolutely no eye focus and stared very blankly never even trying to make eye contact. Even weeks later his left eye still sat higher on his face and his face was very asymmetrical. The left side of his face also drooped with poor muscle tone and without expression. His feedings were extremely difficult and he could not breastfeed well. On top of sucking problems, milk would spew from his nostrils if he was not held in an upright position.
I called into Finn’s pediatrician at 6 weeks of age and told her my concerns of his held tilt and vision. His pediatrician said that the head tilt was torticollis and not uncommon and that the vision problems would resolve as his eyes matured a bit. She said that she would take a look at his 8 week appointment. By his 8 week appointment my concerns and worry were through the roof. I just knew that Finn was not developing normally. He didn’t sleep, he had great difficulty nursing and I had to feed him pumped breast milk from a bottle, and he surely couldn’t see well. All of my concerns and worries were almost dismissed and one of his pediatricians told me to go home, stretch his neck, feed him from a bottle and not worry about his eyes. I chased after her as she left the room and went into her office. I insisted she write a referral for physical therapy and decided to make my own appointment with an eye doctor.
Finn began physical therapy for his torticollis within a couple of weeks and we went to see a ophthalmologist when he was around 3 months old. The ophthalmologist acknowledged immediately that Finn had an eye issue. She was concerned also that his eyes did not seem to abduct out. She was correct. Finn went in for his first MRI at the local children’s hospital. The results did not show any nerve damage or anything else. It was just a mystery. The ophthalmologist sent Finn to a neuro ophthalmologist for a second opinion. The neuro ophthalmologist looked Finn over for about ten minutes and declared he had Moebius Syndrome. Moebius Syndrome is characterized by a complete absence of cranial nerve 6 and 7 movement along this a variety of other symptoms. There is no testing for it. It is just diagnosed with observation of a set of symptoms. I didn’t think Finn had this from day one of his diagnosis and it is clear now that he doesn’t have Mobieus Syndrome because now, Finn has facial movement on the left side of his face. Mobieus Syndrome doesn’t ever get better. The neuron ophthalmologist then referred us to a pediatric neurologist who recommended repeating the brain MRI to include the brainstem and cervical spine. The MRI showed subtle, possibly abnormal, structural abnormality based on an inverted V-shape of the fourth ventricle but no other abnormal findings.
So, we moved on. I came to the realization that Finn’s greatest issues were not his facial asymmetry or his horizontal gaze palsy or his feeding difficulties. Finn’s greatest issue was the torticollis. The torticollis was being aggressively treated yet we did not seem to be getting anywhere with the treatment. When Finn was about 5 months old I had noticed that when I carried him he felt very shifted to his left side . I asked his pediatrician about it and she stated that it was his muscle development and that he was developing more on his left side. This did not sound correct to me, but what did I know. We moved along and Finn was in vision therapy, speech therapy and physical therapy. He didn’t sit up well, he did not crawl and he screamed at night like I was torturing him. I decided to take him to Shriner’s Hospital in Tampa Florida for another opinion. When his appointment time came, he had learned to do an army crawl and he pulled with one arm and pushed off with his big toe. He was also doing a little better job of sitting.
Finn’s first Shriner’s appointment was when he was 11 months old. Sure enough, he was diagnosed with scoliosis. The findings were: T8 to L4 42 degree levoscoliosis. The AP and lateral C-spine x-rays showed no obvious bone abnormalities and the AP spine and pelvis x-rays showed a left thoracolumbar curve of 42 degrees. The hips were well contained and the lateral spine x-ray showed no obvious bone abnormalities and no congenital vertebral anomalies. I was terrified. We were referred to a geneticist to put all of the pieces together because Finn did not have all the classic characteristics of Mobieus syndrome. We were advised to watch and wait to see if the scoliosis progressed. I had absolutely no idea what a beast infantile scoliosis could turn in to. I look back at how naïve I was and how unconcerned Finn’s medical providers seem to be. I just had no idea…
Finn had his genetics appointment and there were no additional findings. At about this time we also began to see a chiropractor, because his MRI had ruled out structural abnormalities. The chiropractor studied Finn up and down. She was determined to make a difference in his life. She worked and worked on his head with cranial sacral therapy to reshape his cranial asymmetry. Little by little we began to see the left side of his face move. Within months of his chiropractic therapy he was smiling a full, normal, toothy smile. He had never been able to move his mouth and face like this and we were so excited and so very hopeful.. I look back on Finn’s first smiles and I think that this was really the first time he had shown some expression of happiness. He had screamed and cried during the night from the time he was born. I knew he was a fighter. His smile told me that he was trying to burst out of his immobile shell.
Finn struggled through the next few months. His head was always going the wrong direction or no direction at all. He was not developing within his normal range and his developmental delays were more noticeable than ever. All of our little friends of the same age were walking, talking and playing but Finn really struggled just to move a few feet. He had trouble rotating his head and that was the only way he could see what was going on around his sides because his eyes did not turn out to look. He could only look forward. We worked so hard. I gave him a massage every night. I rotated and stretched his head. I walked with him, I talked with him. I loved on him like he was all I ever loved. We attended all of his scheduled therapies. He spent so much time just trying to make his body behave as physically normal as possible that he learned nothing else. He just wanted to move!
At 17 months old we returned to Shriner’s Hospital in Tampa. Finn’s AP of the spine showed a left thoracolumbar curve of 60 degrees. The scoliosis had definitely increased from previous films. The vertebral and intervertebral disk spaces were maintained. The bony structures of the pelvis were normal and the femoral heads were within their perspective acetabula. Shriner’s in Florida recommended a brace. They also discussed with me the possibility of needing a distraction rod in the future. I asked if there was any other treatments available for infantile scoliosis. I was told that there were none. Bracing and surgery were the only opinions, or do nothing. Finn was molded for a brace and told to return in 4 weeks. We returned for the brace but there was a problem with getting a good fit and giving Finn correction so Orthotics & Prosthetics wanted to do a Risser cast for a brace mold. They did a mold and made the brace, this was another month, and when that brace was made it did not fit correctly either. So, Finn was molded again with a Risser Cast and a brace was made from the cast. Shriner’s was satisfied with this brace and we were sent home and told to return in four months because they wanted to monitor him because they stated that he may require surgical intervention in the future He measured 40 degrees in the brace.
We went home with that brace. He absolutely could not support his body or his neck in the brace. He laid on the floor mostly and refused to try to do anything. I knew this was not going to work. I had done a little research on my own when the braces were being made and they had told me that he would possibly need surgical intervention. I remembered that there was a method of serial casting that was being practiced at some Shriner’s Hospitals but it was not practiced in Tampa. I went back and found that site. Finn will probably thank me for the rest of his life that I did. It changed his life. ISOP (Infantile Scoliosis Outreach Program) was the only brace that mended my son. It began to heal him the minute I joined the group.
Now, just to give you some background on myself. I am natural to the core. I feed my kids fish oil, pro biotics, and vitamins on a daily basis. They are allowed their share of junk food but eat a natural whole foods diet. My home is as natural as possible and we do not use pesticides or harsh cleaning chemicals. The idea of putting rods in my baby was very uncomfortable to me. I believe in natural health and homeopathic cures when possible. I was really scared to commit to EDF (Elongation, Derotation, Flexion) serial corrective casting, but it was my son’s best alternative to very invasive, repeated surgeries. I worried about if the cast would be uncomfortable, I worried about if he would be to hot in the Florida sun, I worried about what I would do if Finn chocked. I worried about how I would bathe him, how would he do being unable to get wet at the beach or pool. Could he walk in it, could he run in it? Could he just be a little boy in it? Well, I thought about all of this and really looked at my options. He could barely get around as it stood because he was so crippled over with torticollis and low muscle tone. I read and I studied ever story. I knew that Finn did not have a very good chance to get 100% straight because of his degree of curvature, rotation and his age but I decided we just had to try. I made an appointment with the closest physician that was practicing the Mehta Method. This physician was not part of the Shriner’s network but we decided to give him a try anyway. We went to the appointment and the physician agreed to cast Finn. The next morning Finn went in for casting. About an hour after Finn went into the OR the physician came out and said that he could not cast Finn. He said that I should take him to get growth rods immediately. I was absolutely devastated. I lost all hope. I cried for days. When I returned home with Finn I posted on the ISOP support group that Finn had been unsuccessful in our casting attempt. I learned that some doctors are not following the exact recommendations of EDF casting and the Mehta Method. He was modifying the plaster jacket by not using shoulder straps in all cases. He did have kids with low curves that were achieving correction but this modified method without the support of shoulder straps was not going to work for Finn and his high thoracic curves. He just had too many neck issues going on and he needed the shoulder straps to hold his shoulder area and chest cavity in place. I was encouraged by another mother on the group to get another opinion. The mother suggested the Shriner’s in Chicago. I gave them a call and sent all of Finn’s medical documentation up to be reviewed. They called and told us to come on up. I was so nervous and excited. We went ASAP.
On our initial visit Finn’s x-rays showed that he had progressed to nearly 90 degrees. It had been less than four months since our last x-rays and the curve was progressing like wildfire now. He could hardly stand at this point. His overall function was almost as bad as it had ever been. He just could not develop like he needed to because all of his energy and focus was on trying to support his body. The attending physician noted that he was very flexible and in traction x rays he looked much better. The physician said he would try to cast him the next day. I was not going to set myself up again for disappointment so I just did not get very excited. The next day Finn was casted. After the casting, his physician came out and told me he “looked good”. Looked good I thought, oh my goodness, could this be true? I was beyond words. I was crying with relief. He was casted down to the mid 30’s. This was achievable because the doctor treated my child individually, had EDF experience and knew the importance of shoulder straps for curves above T-9.
Finn came out of recovery and we wheeled him down to his room. His cast was taped and trimmed. I picked him up and put him on the ground. He was a little disorientated and a bit uncomfortable and unsure of what had just gone on. He held his body tall and strong for the first time in his life. He laughed, and he moved, and he tried to walk. I packed him up that afternoon and went back to Florida. With in the next few days Finn became very comfortable with his new accessory. Once he adjusted to the weight of the cast he was full steam ahead. Finn was amazing. The cast allowed him to stand without slumping. He could walk and move freely. He immediately started doing things I had never seen him do. Finn was a new kid. It was the beginning for him. It was the beginning of his new life where he had an opportunity to learn without pain, where he had the opportunity to be the same as his peers and run with the wind, and where he had the opportunity to focus on something else than just trying to standing up.
Finn has received good correction in his casts. He just went in for number 7. I have never been one for numbers or degrees. I have always known that Finn will most likely never get full correction like some of the younger kids with less severe curves. I choose not to ask what his numbers are. I know he is still above 50 degrees but he is well below 90 degrees. I also know that he gets down to about 28 degrees in his cast. I just really don’t need to know numbers though. I am not focused on that. I am focused on the new chance for life that Early Treatment w/ properly applied EDF casting and the Mehta Method has given my child. I am concerned for his overall development. I want him to develop in all the ways his peers have had the opportunity to develop. I just want Finn to have the chance of a the most normal life possible, one that is free of pain and full of opportunity to grow, develop, and explore in this world that is so full of life. And you know what??? He is, and the reason he is full of life is because of Mehta casting and the absolute best medical team at the Shriner’s Hospital in Chicago.
Finn continues to achieve success. He just turned three and is doing remarkably well. His vision has improved and he has learned to rotate his head to see what surrounds him. His facial palsy is almost nonexistent. He runs, and he plays and he has the most inspiring, infectious laugh. He is always in trouble for getting into something or climbing on something. He is the pillar of strength and determination. At the end of the day I know that he most likely will require surgical intervention but the casting has given him the opportunity to grow a little more , develop a little more and explore life a little more. I could not ask for anything more.

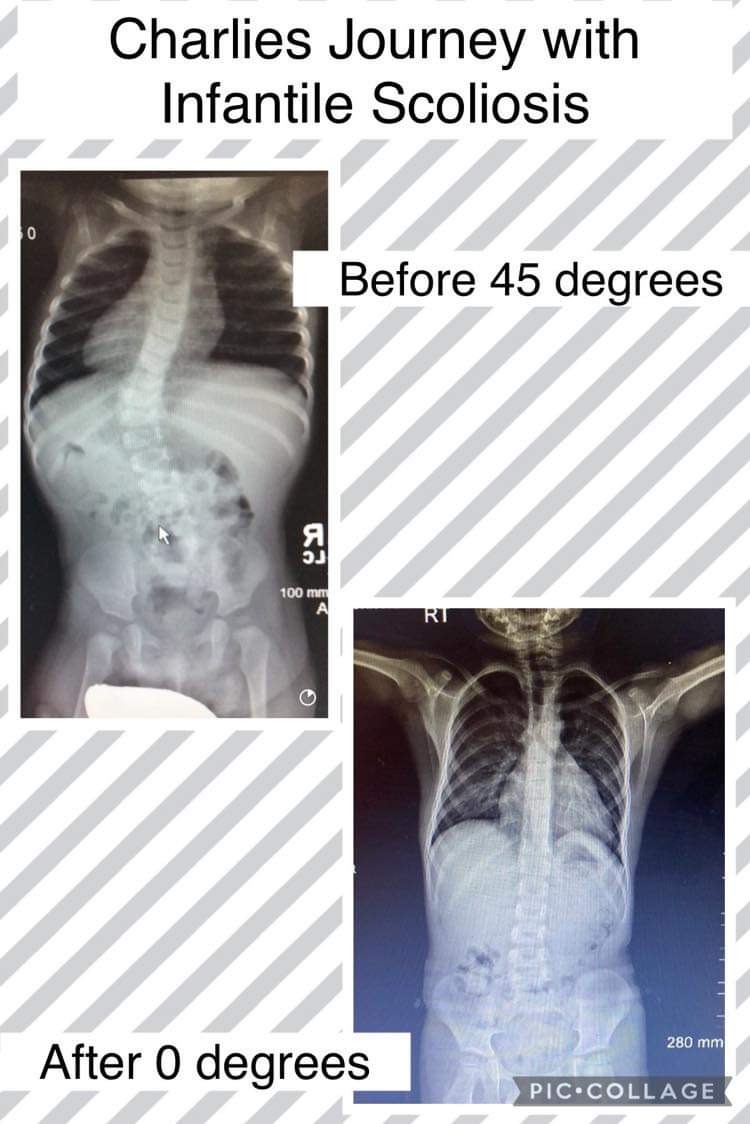
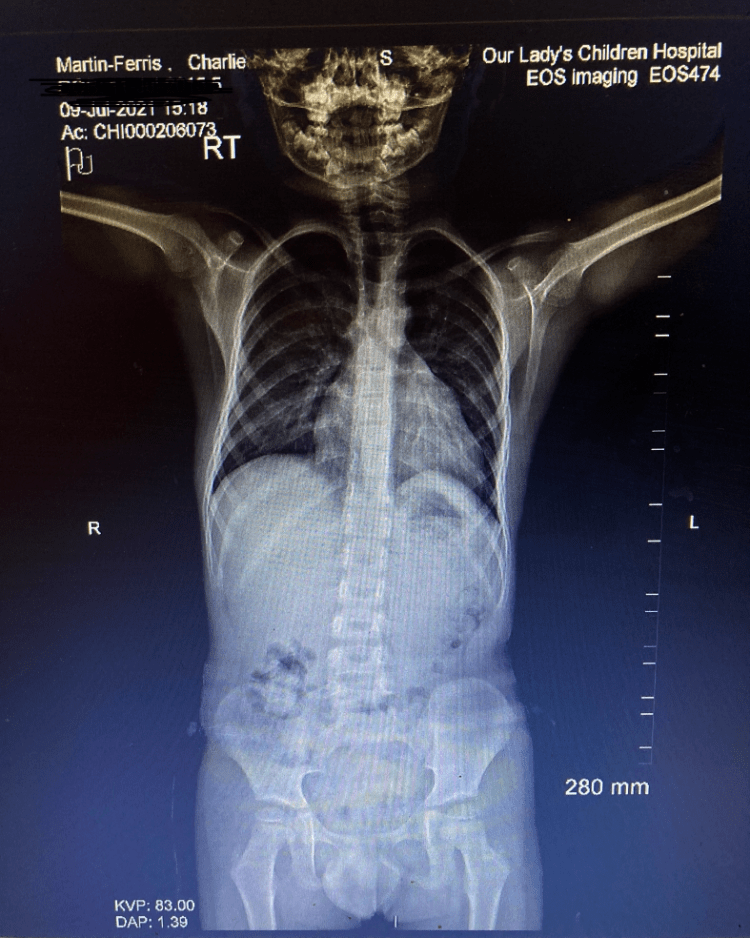

 For thousands of families across the world and for ACCO, 2005 was one of those remarkable times when we experienced a significant sea change in the treatment of very young children with a diagnosis of life threatening Progressive Infantile Scoliosis.
For thousands of families across the world and for ACCO, 2005 was one of those remarkable times when we experienced a significant sea change in the treatment of very young children with a diagnosis of life threatening Progressive Infantile Scoliosis.


 Maggie’s surgery was scheduled a couple days after her fourth birthday. We told her staying in the hospital would mean as many movies as she wanted – she was very excited. The surgery took three hours, three nerve-wracking hours, full of pacing, staring at each other, and mindlessly surfing the internet. She metabolized the anesthesia very quickly, and woke up fast and disoriented in the PICU, without us there. When we were finally allowed back, it took my wife a long time to calm Maggie down. Sleeping in hospitals is the absolute worst: two days in the PICU, and 4 more in the recovery room put a huge strain on my wife, who would not leave. Maggie’s condition was sub-par, she was unable to move her right arm (fingers moved though), her pain was high, and we were discharged with her hardly walking. A slow couple of weeks saw her going back to preschool an hour at a time, and some increased right arm movement. Then everything went bad, very bad…
Maggie’s surgery was scheduled a couple days after her fourth birthday. We told her staying in the hospital would mean as many movies as she wanted – she was very excited. The surgery took three hours, three nerve-wracking hours, full of pacing, staring at each other, and mindlessly surfing the internet. She metabolized the anesthesia very quickly, and woke up fast and disoriented in the PICU, without us there. When we were finally allowed back, it took my wife a long time to calm Maggie down. Sleeping in hospitals is the absolute worst: two days in the PICU, and 4 more in the recovery room put a huge strain on my wife, who would not leave. Maggie’s condition was sub-par, she was unable to move her right arm (fingers moved though), her pain was high, and we were discharged with her hardly walking. A slow couple of weeks saw her going back to preschool an hour at a time, and some increased right arm movement. Then everything went bad, very bad…











 When their beautiful 15 month old daughter, Karleigh, was diagnosed with progressive infantile scoliosis (PIS), Kim Westmiller and her husband had no idea what they were up against. Fortunately, they were able to connect with Heather Hyatt Montoya and the Infantile Scoliosis Outreach Program (ISOP). Through Heather and ISOP, they found answers to their questions and the resources that led them to Early Treatment with Mehta Casting. These specialized EDF casts are applied every 8 weeks and continue to have a straightening effect on 3 year old Karleigh’s spine.
When their beautiful 15 month old daughter, Karleigh, was diagnosed with progressive infantile scoliosis (PIS), Kim Westmiller and her husband had no idea what they were up against. Fortunately, they were able to connect with Heather Hyatt Montoya and the Infantile Scoliosis Outreach Program (ISOP). Through Heather and ISOP, they found answers to their questions and the resources that led them to Early Treatment with Mehta Casting. These specialized EDF casts are applied every 8 weeks and continue to have a straightening effect on 3 year old Karleigh’s spine.










{kind=link}
{kind=link}